Department of Radiation Oncology, H. Lee Moffitt Cancer Center, Tampa, FL, USA.
J Thorac Oncol. 2012 May;7(5):906-12. doi: 10.1097/JTO.0b013e31824c7bed.
The specific aims of the study were to evaluate the 2-year overall survival (OS) and progression-free survival (PFS), toxicity profile, and best objective response rate in patients with locally advanced, clinically unresectable esophageal cancer receiving cetuximab, cisplatin, irinotecan, and thoracic radiotherapy (TRT) within a multi-institutional cooperative-group setting.
Eligible patients (cT4 M0 or medically unresectable, biopsy proven, and noncervical esophageal cancer) were to receive four 21-day cycles of cetuximab 400 mg/m (day 1, cycle 1), cetuximab 250 mg/m (day 8, 15, cycle 1; then days 1, 8, and 15 for subsequent cycles), cisplatin 30 mg/m (days 1 and 8, all cycles), and irinotecan 65 mg/m (days 1 and 8, all cycles). TRT was administered at 1.8 Gy in 28 daily fractions to a total dose of 50.4 Gy, to begin with on day 1 of cycle 3. The primary endpoint was 2-year OS, with an accrual goal of 75 patients with adenocarcinoma.
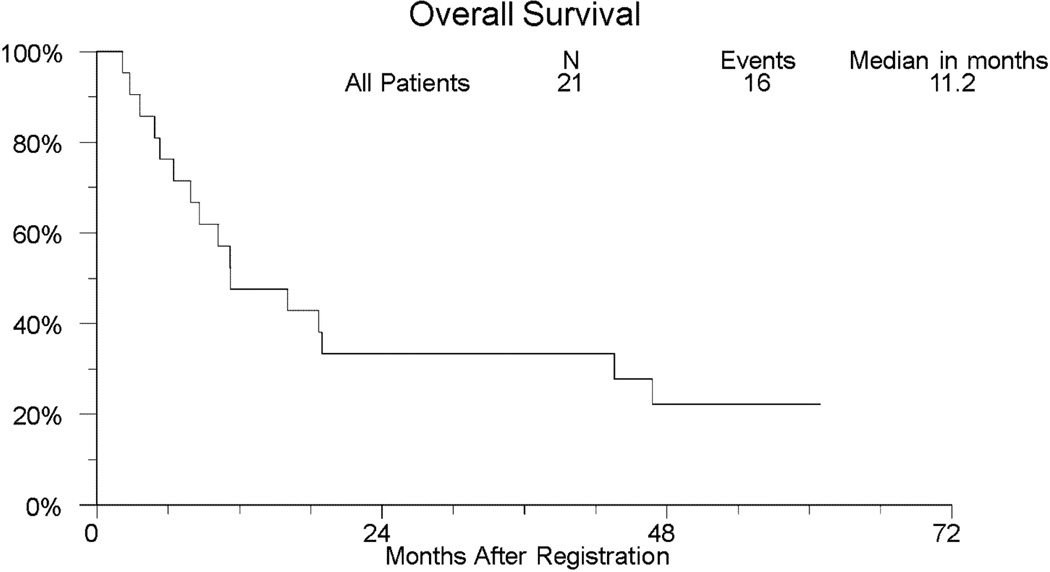
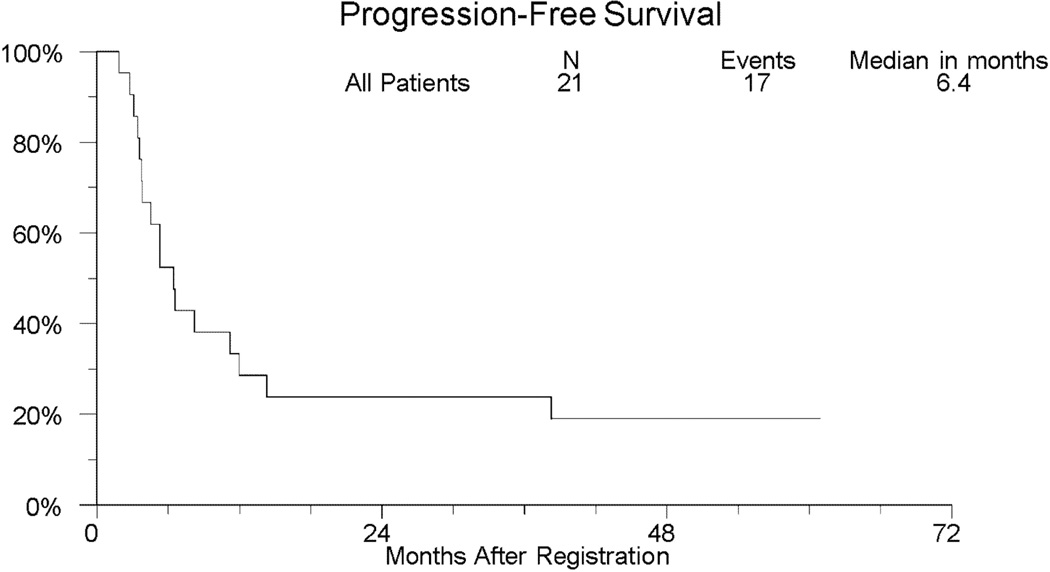
The study was closed because of slow accrual, with 21 eligible patients (11 squamous, 10 adenocarcinoma) enrolled from May 2005 to September 2007. Two-year OS and PFS (95% confidence interval [CI]) were 33.3% (14.6-57.0%) and 23.8% (8.2-47.2%), respectively. Kaplan-Meier estimates of median (95% CI) OS and PFS were 11.2 (6.4-43.6) and 6.4 (3.7-12.0) months, respectively. The overall response rate (95% CI) among 17 evaluable patients was 17.6% (3.8-43.4%), including 6% confirmed complete responders and 12% unconfirmed partial responders. Two deaths resulted from protocol treatment (sudden death and gastrointestinal necrosis). Ten (47.6%) and 6 (28.6%) patients had grade-3 or -4 toxicity, respectively: 52.4% were hematologic, 23.8% had fatigue, 19.0% had nausea, 19.0% had dehydration, and 19.0% had anorexia.
Concomitant cetuximab, cisplatin, irinotecan, and TRT were poorly tolerated in the first North American cooperative group trial testing this regimen for locally advanced esophageal cancer as treatment-related mortality approached 10%. Single-institution phase-II cetuximab-based combined modality trials have yielded encouraging results in preliminary analyses. The SWOG GI Committee endorses enrollment to open clinical trials to clarify the therapeutic ratio of cetuximab-based combined modality approaches for esophageal cancer.
本研究的具体目的是评估在多机构合作组环境下,局部晚期、临床不可切除的食管鳞癌和腺癌患者接受西妥昔单抗、顺铂、伊立替康和胸部放射治疗(TRT)的 2 年总生存(OS)和无进展生存(PFS)、毒性谱和最佳客观缓解率。
符合条件的患者(cT4 M0 或医学上不可切除,经活检证实且非颈段食管癌)接受 4 个 21 天周期的西妥昔单抗 400mg/m²(第 1 天,第 1 周期)、西妥昔单抗 250mg/m²(第 8 天和第 15 天,第 1 周期;然后第 1、8 和 15 天用于后续周期)、顺铂 30mg/m²(所有周期的第 1 和第 8 天)和伊立替康 65mg/m²(所有周期的第 1 和第 8 天)。TRT 从第 3 周期第 1 天开始,在 28 个每日剂量中以 1.8Gy 给药,总剂量为 50.4Gy。主要终点是 2 年 OS,腺癌的入组目标为 75 例。
由于入组缓慢,该研究于 2005 年 5 月至 2007 年 9 月结束,共纳入 21 例符合条件的患者(11 例鳞癌,10 例腺癌)。2 年 OS 和 PFS(95%置信区间[CI])分别为 33.3%(14.6-57.0%)和 23.8%(8.2-47.2%)。17 例可评估患者的中位(95%CI)OS 和 PFS 分别为 11.2(6.4-43.6)和 6.4(3.7-12.0)个月。17 例可评估患者的总体缓解率(95%CI)为 17.6%(3.8-43.4%),包括 6%的确认完全缓解者和 12%的未确认部分缓解者。2 例患者死于治疗相关(猝死和胃肠道坏死)。10 例(47.6%)和 6 例(28.6%)患者出现 3 级或 4 级毒性,分别为:52.4%为血液学毒性,23.8%为疲劳,19.0%为恶心,19.0%为脱水,19.0%为厌食。
在北美首个合作组试验中,西妥昔单抗、顺铂、伊立替康和 TRT 联合治疗局部晚期食管癌耐受性较差,治疗相关死亡率接近 10%。单机构的Ⅱ期西妥昔单抗为基础的联合治疗试验在初步分析中取得了令人鼓舞的结果。SWOG GI 委员会支持开展开放性临床试验,以明确西妥昔单抗为基础的联合治疗方法治疗食管癌的治疗比值。