School of Medicine, University of Western Sydney, Narellan Road, Campbelltown, NSW, Australia.
BMC Public Health. 2012 Apr 10;12:281. doi: 10.1186/1471-2458-12-281.
Heart disease is a leading cause of the gap in burden of disease between Aboriginal and non-Aboriginal Australians. Our study investigated short- and long-term mortality after admission for Aboriginal and non-Aboriginal people admitted with acute myocardial infarction (AMI) to public hospitals in New South Wales, Australia, and examined the impact of the hospital of admission on outcomes.
Admission records were linked to mortality records for 60047 patients aged 25-84 years admitted with a diagnosis of AMI between July 2001 and December 2008. Multilevel logistic regression was used to estimate adjusted odds ratios (AOR) for 30- and 365-day all-cause mortality.
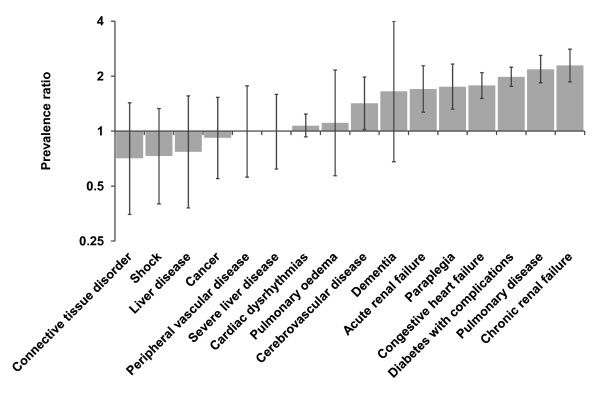
Aboriginal patients admitted with an AMI were younger than non-Aboriginal patients, and more likely to be admitted to lower volume, remote hospitals without on-site angiography. Adjusting for age, sex, year and hospital, Aboriginal patients had a similar 30-day mortality risk to non-Aboriginal patients (AOR: 1.07; 95% CI 0.83-1.37) but a higher risk of dying within 365 days (AOR: 1.34; 95% CI 1.10-1.63). The latter difference did not persist after adjustment for comorbid conditions (AOR: 1.12; 95% CI 0.91-1.38). Patients admitted to more remote hospitals, those with lower patient volume and those without on-site angiography had increased risk of short and long-term mortality regardless of Aboriginal status.
Improving access to larger hospitals and those with specialist cardiac facilities could improve outcomes following AMI for all patients. However, major efforts to boost primary and secondary prevention of AMI are required to reduce the mortality gap between Aboriginal and non-Aboriginal people.
心脏病是导致澳大利亚原住民和非原住民之间疾病负担差距的主要原因。我们的研究调查了在澳大利亚新南威尔士州公立医院因急性心肌梗死(AMI)入院的原住民和非原住民患者的短期和长期死亡率,并研究了入院医院对结果的影响。
将 2001 年 7 月至 2008 年 12 月期间诊断为 AMI 的 60047 名 25-84 岁患者的入院记录与死亡率记录进行了关联。使用多水平逻辑回归来估计 30 天和 365 天全因死亡率的调整优势比(AOR)。
因 AMI 入院的原住民患者比非原住民患者年轻,更有可能被收入容量较低、没有现场血管造影的偏远医院。在调整年龄、性别、年份和医院后,原住民患者的 30 天死亡率与非原住民患者相似(AOR:1.07;95%CI 0.83-1.37),但在 365 天内死亡的风险更高(AOR:1.34;95%CI 1.10-1.63)。在调整合并症后,这种差异并不存在(AOR:1.12;95%CI 0.91-1.38)。无论原住民身份如何,入住偏远医院、患者数量较少且没有现场血管造影的患者,短期和长期死亡率都有增加的风险。
改善对较大医院和具有专科心脏设施的医院的获取途径,可以改善所有患者的 AMI 后结局。然而,需要做出重大努力来加强 AMI 的一级和二级预防,以缩小原住民和非原住民之间的死亡率差距。