Department of Surgery, Maastricht University Medical Center, Maastricht, The Netherlands.
PLoS One. 2012;7(4):e34491. doi: 10.1371/journal.pone.0034491. Epub 2012 Apr 4.
Inadequate flow enhancement on the one hand, and excessive flow enhancement on the other hand, remain frequent complications of arteriovenous fistula (AVF) creation, and hamper hemodialysis therapy in patients with end-stage renal disease. In an effort to reduce these, a patient-specific computational model, capable of predicting postoperative flow, has been developed. The purpose of this study was to determine the accuracy of the patient-specific model and to investigate its feasibility to support decision-making in AVF surgery.
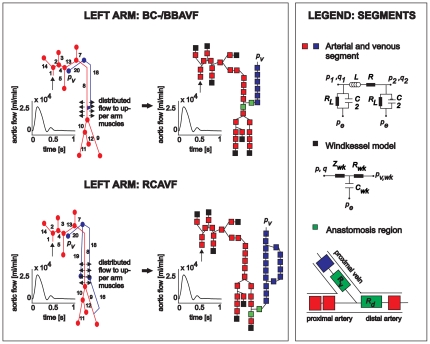
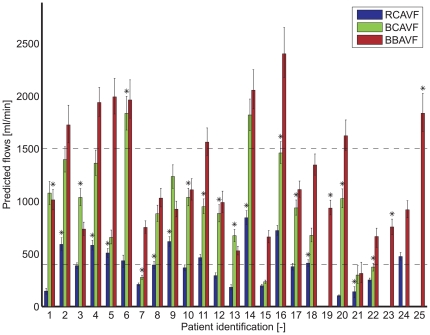
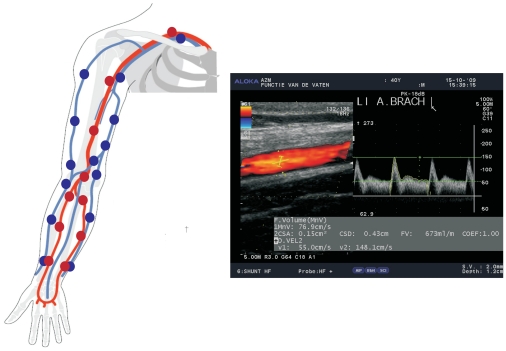
Patient-specific pulse wave propagation models were created for 25 patients awaiting AVF creation. Model input parameters were obtained from clinical measurements and literature. For every patient, a radiocephalic AVF, a brachiocephalic AVF, and a brachiobasilic AVF configuration were simulated and analyzed for their postoperative flow. The most distal configuration with a predicted flow between 400 and 1500 ml/min was considered the preferred location for AVF surgery. The suggestion of the model was compared to the choice of an experienced vascular surgeon. Furthermore, predicted flows were compared to measured postoperative flows.
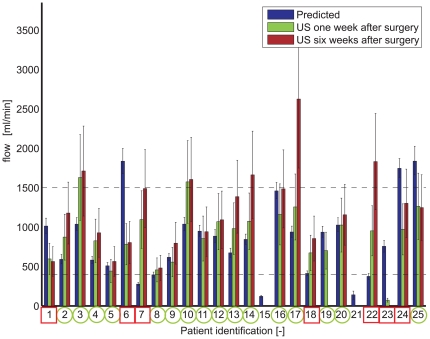
Taken into account the confidence interval (25(th) and 75(th) percentile interval), overlap between predicted and measured postoperative flows was observed in 70% of the patients. Differentiation between upper and lower arm configuration was similar in 76% of the patients, whereas discrimination between two upper arm AVF configurations was more difficult. In 3 patients the surgeon created an upper arm AVF, while model based predictions allowed for lower arm AVF creation, thereby preserving proximal vessels. In one patient early thrombosis in a radiocephalic AVF was observed which might have been indicated by the low predicted postoperative flow.
Postoperative flow can be predicted relatively accurately for multiple AVF configurations by using computational modeling. This model may therefore be considered a valuable additional tool in the preoperative work-up of patients awaiting AVF creation.
一方面,动静脉瘘(AVF)创建后的血流增强不足,另一方面,血流增强过度,仍然是常见的并发症,会阻碍终末期肾病患者的血液透析治疗。为了减少这些并发症,已经开发出一种能够预测术后流量的患者特异性计算模型。本研究的目的是确定该患者特异性模型的准确性,并研究其在辅助动静脉瘘手术决策中的可行性。
为 25 名等待动静脉瘘创建的患者创建了患者特异性脉搏波传播模型。模型输入参数是从临床测量和文献中获得的。对每位患者,模拟了头臂静脉动静脉瘘、肱动脉动静脉瘘和肱动脉-正中静脉动静脉瘘三种配置,并对其术后流量进行了分析。将预测流量在 400 至 1500ml/min 之间的最远端配置视为动静脉瘘手术的首选位置。将模型的建议与经验丰富的血管外科医生的选择进行了比较。此外,还比较了预测流量与术后测量的流量。
考虑到置信区间(第 25 个和第 75 个百分位数区间),在 70%的患者中观察到预测和术后测量的流量之间存在重叠。在 76%的患者中,上臂和前臂配置之间的区分相似,而两种上臂动静脉瘘配置之间的区分更加困难。在 3 名患者中,外科医生创建了上臂动静脉瘘,而基于模型的预测允许创建前臂动静脉瘘,从而保留了近端血管。在一名患者中,观察到头臂静脉动静脉瘘早期血栓形成,这可能是由于预测的术后流量低而导致的。
通过使用计算建模,可以相对准确地预测多种动静脉瘘配置的术后流量。因此,该模型可以被认为是等待动静脉瘘创建的患者术前评估的有价值的附加工具。