Department of Internal Medicine and Cardiology, University Hospital Brno and Faculty of Medicine, Masaryk University, Brno, Czech Republic.
BMC Cardiovasc Disord. 2012 Apr 25;12:31. doi: 10.1186/1471-2261-12-31.
Older age, as a factor we cannot affect, is consistently one of the main negative prognostic values in patients with acute myocardial infarction. One of the most powerful factors that improves outcomes in patients with acute coronary syndromes is the revascularization preferably performed by percutaneous coronary intervention. No data is currently available for the role of age in large groups of consecutive patients with PCI as the nearly sole method of revascularization in AMI patients. The aim of this study was to analyze age-related differences in treatment strategies, results of PCI procedures and both in-hospital and long-term outcomes of consecutive patients with acute myocardial infarction.
Retrospective multicenter analysis of 3814 consecutive acute myocardial infarction patients divided into two groups according to age (1800 patients ≤ 65 years and 2014 patients > 65 years). Significantly more older patients had a history of diabetes mellitus and previous myocardial infarctions.
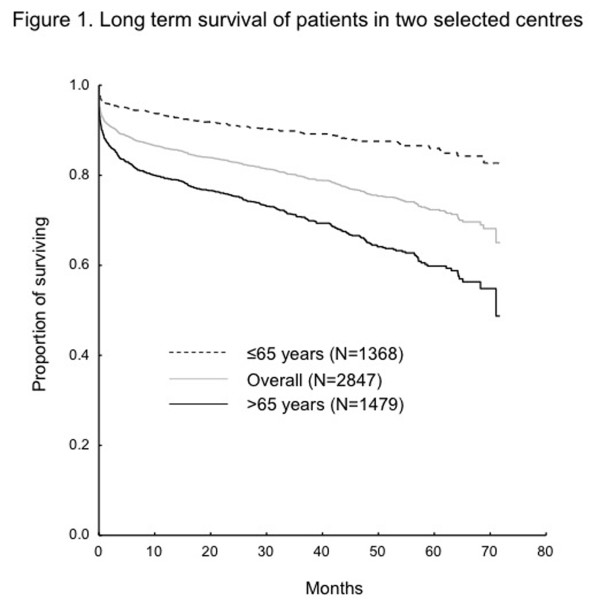
The older population had a significantly lower rate of coronary angiographies (1726; 95.9% vs. 1860; 92.4%, p < 0.0001), PCI (1541; 85.6% vs. 1505; 74.7%, p < 0.001), achievement of optimal final TIMI flow 3 (1434; 79.7% vs. 1343; 66.7%, p < 0.001) and higher rate of unsuccessful reperfusion with final TIMI flow 0-1 (46; 2.6% vs. 78; 3.9%, p = 0.022). A total of 217 patients (5.7%) died during hospitalization, significantly more often in the older population (46; 2.6% vs. 171; 8.5%, p < 0.001). The long-term mortality (data for 2847 patients from 2 centers) was higher in the older population as well (5 years survival: 86.1% vs. 59.8%). Though not significantly different and in contrast with PCI, the presence of diabetes mellitus, previous MI, final TIMI flow and LAD, as the infarct-related artery, had relatively lower impact on the older patients. Severe heart failure on admission (Killip III-IV) was associated with the worst prognosis in the whole group of patients, though its significance was higher in the youngers (HR 6.04 vs. 3.14, p = 0.051 for Killip III and 12.24 vs. 5.65, p = 0.030 for Killip IV). We clearly demonstrated age as a strong discriminator for the whole population of AMI patients.
In a consecutive AMI population, the older group (>65 years) was associated with a less pronounced impact of risk factors on long-term outcome. To ascertain the coronary anatomy by coronary angiography and proceed to PCI if suitable regardless of age is crucial in all patients, though the primary success rate of PCI in the older age is lower. Age, when viewed as a risk factor, was a dominant discriminating factor in all patients.
年龄是一个不可改变的因素,在急性心肌梗死患者中一直是主要的负面预后因素之一。在急性冠状动脉综合征患者中,改善预后的最有力因素之一是通过经皮冠状动脉介入治疗(PCI)进行血运重建。目前尚无数据可用于年龄较大的患者群体,这些患者几乎仅接受 PCI 作为 AMI 患者的血运重建方法。本研究旨在分析年龄相关的治疗策略差异、PCI 手术结果以及急性心肌梗死患者的住院和长期预后。
回顾性多中心分析了 3814 例连续急性心肌梗死患者,根据年龄分为两组(1800 例患者≤65 岁和 2014 例患者>65 岁)。年龄较大的患者有更多的糖尿病和既往心肌梗死病史。
老年组的冠状动脉造影(1726 例;95.9%比 1860 例;92.4%,p<0.0001)、PCI(1541 例;85.6%比 1505 例;74.7%,p<0.001)、达到最佳最终 TIMI 血流 3 级(1434 例;79.7%比 1343 例;66.7%,p<0.001)的比例明显较低,而最终 TIMI 血流 0-1 级的无复流率较高(46 例;2.6%比 78 例;3.9%,p=0.022)。共有 217 例(5.7%)患者在住院期间死亡,老年组明显更多(46 例;2.6%比 171 例;8.5%,p<0.001)。老年组的长期死亡率(来自 2 个中心的 2847 例患者的数据)也更高(5 年生存率:86.1%比 59.8%)。尽管与 PCI 相比,糖尿病、既往心肌梗死、最终 TIMI 血流和左前降支(LAD)作为梗死相关动脉的存在对老年患者的影响并不显著,但也相对较低。入院时严重心力衰竭(Killip III-IV 级)与全组患者的预后最差相关,尽管在年轻人中其意义更高(HR 6.04 比 3.14,p=0.051,Killip III 级;HR 12.24 比 5.65,p=0.030,Killip IV 级)。我们清楚地证明了年龄是 AMI 患者群体的一个强有力的判别因素。
在连续的 AMI 人群中,年龄较大(>65 岁)组与长期预后的风险因素的影响程度较轻相关。在所有患者中,通过冠状动脉造影确定冠状动脉解剖结构并进行 PCI,如果合适的话,这是至关重要的,尽管老年患者的 PCI 初次成功率较低。年龄作为一个危险因素,在所有患者中都是一个主要的判别因素。