Department of Neurological, Neuropsychological, Morphological and Movement Sciences, Section of Clinical Neurology, University of Verona, Piazzale L.A. Scuro 10, 37134, Verona, Italy.
J Headache Pain. 2012 Jul;13(5):339-49. doi: 10.1007/s10194-012-0445-6. Epub 2012 Apr 27.
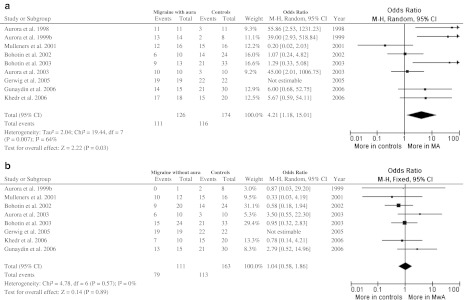
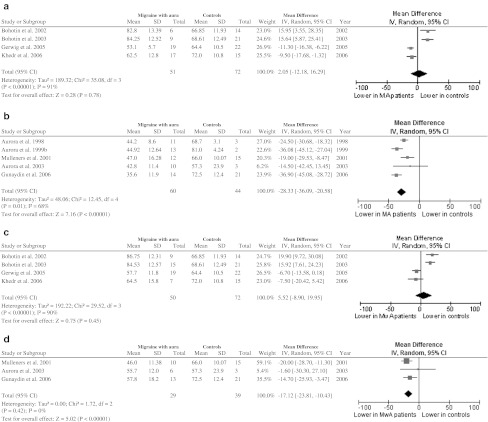
We systematically reviewed the literature to evaluate the prevalence of phosphenes and the phosphene threshold (PT) values obtained during single-pulse transcranial magnetic stimulation (TMS) in adults with migraine. Controlled studies measuring PT by single-pulse TMS in adults with migraine with or without aura (MA, MwA) were systematically searched. Prevalence of phosphenes and PT values were assessed calculating mean difference (MD) and odds ratio (OR) with 95 % confidence intervals (CI). Ten trials (277 migraine patients and 193 controls) were included. Patients with MA had statistically significant lower PT compared with controls when a circular coil was used (MD -28.33; 95 % CI -36.09 to -20.58); a similar result was found in MwA patients (MD -17.12; 95 % CI -23.81 to -10.43); using a figure-of-eight coil the difference was not statistically significant. There was a significantly higher phosphene prevalence in MA patients compared with control subjects (OR 4.21; 95 % CI 1.18-15.01). No significant differences were found either in phosphene reporting between patients with MwA and controls, or in PT values obtained with a figure-of-eight coil in MA and MwA patients versus controls. Overall considered, these results support the hypothesis of a primary visual cortex hyper-excitability in MA, providing not enough evidence for MwA. A significant statistical heterogeneity reflects clinical and methodological differences across studies, and higher temporal variabilities among PT measurements over time, related to unstable excitability levels. Patients should therefore be evaluated in the true interictal period with an adequate headache-free interval. Furthermore, skull thickness and ovarian cycle should be assessed as possible confounding variables, and sham stimulation should be performed to reduce the rate of false positives. Phosphene prevalence alone cannot be considered a measure of cortical excitability, but should be integrated with PT evaluation.
我们系统地回顾了文献,以评估偏头痛成人单次经颅磁刺激(TMS)时出现光幻视的发生率和光幻视阈值(PT)值。系统地搜索了测量偏头痛成人(有或无先兆偏头痛,MA 和 MwA)PT 的单脉冲 TMS 对照研究。使用均数差(MD)和 95%置信区间(CI)评估光幻视发生率和 PT 值。纳入了 10 项试验(277 例偏头痛患者和 193 例对照)。使用圆形线圈时,MA 患者的 PT 明显低于对照组(MD -28.33;95%CI -36.09 至 -20.58);MwA 患者也有类似的结果(MD -17.12;95%CI -23.81 至 -10.43);使用 8 字形线圈时,差异无统计学意义。与对照组相比,MA 患者的光幻视发生率明显更高(OR 4.21;95%CI 1.18-15.01)。MwA 患者与对照组之间,或 MA 和 MwA 患者与对照组之间,使用 8 字形线圈时,光幻视报告或 PT 值均无显著差异。总体而言,这些结果支持 MA 中初级视觉皮层兴奋性过高的假说,为 MwA 提供的证据不足。统计学异质性显著反映了研究之间的临床和方法学差异,以及随时间推移 PT 测量的时间变异性更高,这与不稳定的兴奋性水平有关。因此,患者应在真正的发作间期,在足够的无头痛间隔期进行评估。此外,应评估颅骨厚度和卵巢周期作为可能的混杂变量,并进行假刺激以降低假阳性率。光幻视的发生率本身不能作为皮质兴奋性的衡量标准,而应与 PT 评估相结合。