Li Jianjie, Qu Lili, Wei Xing, Gao Hongjun, Wang Weixia, Qin Haifeng, Tang Chuanhao, Guo Wanfeng, Wang Hong, Liu Xiaoqing
Department of Pulmonary Neoplasms internal medicine, Affiliated Hospital of Academy of the Military Medical Science, Beijing 100071, China.
Zhongguo Fei Ai Za Zhi. 2012 May;15(5):299-304. doi: 10.3779/j.issn.1009-3419.2012.05.09.
It has been proven that epidermal growth factor receptor-tyrosine kinase inhibitor (EGFR-TKI) significantly benefits advanced non-small cell lung cancer (NSCLC) patients harboring EGFR mutations in progression-free survival time with better tolerance. This study is undertaken to analyze efficacy and tolerance of advanced NSCLC patients harboring EGFR mutations taking EGFR-TKI as a first-line therapy.
Tumor samples from 54 patients with advanced NSCLC were examined for EGFR activating mutations (deletion mutation in exon 19 and the L858R point mutation in exon 21) by direct sequencing. The patients were first-line treated with oral administration of EGFR-TKI until disease progression. The efficacy and adverse events were observed, and survival was followed up.
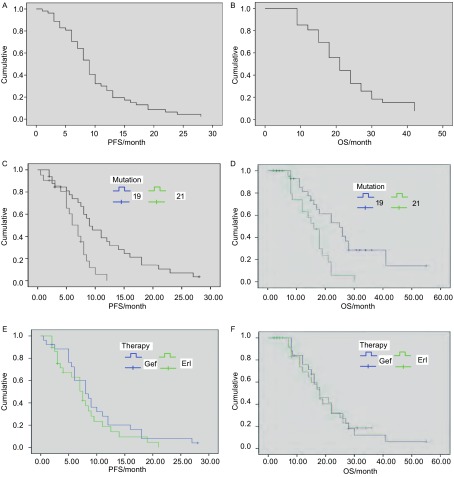
Among the patients, 61% (33 of 54) had EGFR exon 19 deletion, and 39% (21 of 54) had EGFR L858R point mutation. All patients received first-line TKI therapy. The total response rate was 96%, median progression free survival (PFS) was 8.3 months and median survival was 19.5 months. The patients with EGFR exon 19 deletion had significantly longer median PFS (9 versus 7 months, P=0.002) and longer median overall survival (OS)(25 versus 16 months, P=0.001) than patients with EGFR L858R point mutation. There is no significance in efficacy between gefitinib and erlotinib, and gefitinib is safer than erlotinib. The most common adverse events were rash and diarrhea. Two (4%) grade 4 skin toxity effects, two (4%) grade 3 aminotransferase level elevations, and one (1) grade 3 stomatitis were observed.
The first-line EGFR-TKI treatment in advanced NSCLC patients harboring EGFR mutations is efficient and safe, which is more efficient in patients with EGFR exon 19 deletion than those with EGFR L858R mutation.
已证实表皮生长因子受体酪氨酸激酶抑制剂(EGFR-TKI)可显著延长携带EGFR突变的晚期非小细胞肺癌(NSCLC)患者的无进展生存期,且耐受性较好。本研究旨在分析以EGFR-TKI作为一线治疗方案的携带EGFR突变的晚期NSCLC患者的疗效和耐受性。
采用直接测序法检测54例晚期NSCLC患者肿瘤样本中的EGFR激活突变(外显子19缺失突变和外显子21的L858R点突变)。患者接受口服EGFR-TKI一线治疗,直至疾病进展。观察疗效和不良事件,并进行生存随访。
患者中,61%(54例中的33例)存在EGFR外显子19缺失,39%(54例中的21例)存在EGFR L858R点突变。所有患者均接受一线TKI治疗。总缓解率为96%,中位无进展生存期(PFS)为8.3个月,中位生存期为19.5个月。与携带EGFR L858R点突变的患者相比,存在EGFR外显子19缺失的患者中位PFS显著更长(9个月对7个月,P = 0.002),中位总生存期(OS)更长(25个月对16个月,P = 0.001)。吉非替尼和厄洛替尼在疗效上无显著差异,且吉非替尼比厄洛替尼更安全。最常见的不良事件为皮疹和腹泻。观察到2例(4%)4级皮肤毒性反应、2例(4%)3级转氨酶水平升高和1例(1%)3级口腔炎。
对于携带EGFR突变的晚期NSCLC患者,一线EGFR-TKI治疗有效且安全,对于存在EGFR外显子19缺失的患者比存在EGFR L858R突变的患者更有效。