Department of Gastroenterology, Tong Ren Hospital of Wuhan University, Wuhan, Hubei, People's Republic of China.
PLoS One. 2012;7(5):e37614. doi: 10.1371/journal.pone.0037614. Epub 2012 May 22.
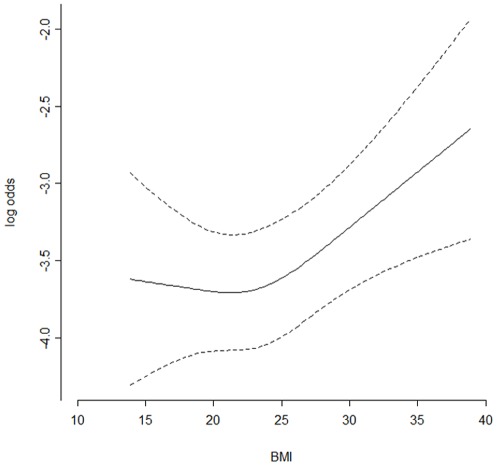
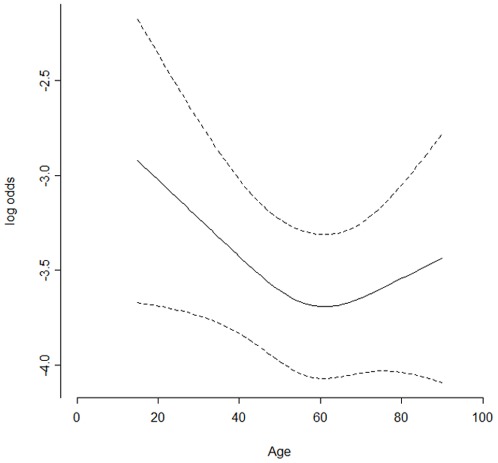
Hypoxemia is the most common adverse event that happened during gastrointestinal endoscopy. To estimate risk of hypoxemia prior to endoscopy, American Society of Anesthesiology (ASA) classification scores were used as a major predictive factor. But the accuracy of ASA scores for predicting hypoxemia incidence was doubted here, considering that the classification system ignores much information about general health status and fitness of patient that may contribute to hypoxemia. In this retrospective review of clinical data collected prospectively, the data on 4904 procedures were analyzed. The Pearson's chi-square test or the Fisher exact test was employed to analyze variance of categorical factors. Continuous variables were statistically evaluated using t-tests or Analysis of variance (ANOVA). As a result, only 245 (5.0%) of the enrolled 4904 patients were found to present hypoxemia during endoscopy. Multivariable logistic regressions revealed that independent risk factors for hypoxemia include high BMI (BMI 30 versus 20, Odd ratio: 1.52, 95% CI: 1.13-2.05; P = 0.0098), hypertension (Odd ratio: 2.28, 95% CI: 1.44-3.60; P = 0.0004), diabetes (Odd ratio: 2.37, 95% CI: 1.30-4.34; P = 0.005), gastrointestinal diseases (Odd ratio: 1.77, 95% CI: 1.21-2.60; P = 0.0033), heart diseases (Odd ratio: 1.97, 95% CI: 1.06-3.68; P = 0.0325) and the procedures that combined esophagogastroduodenoscopy (EGD) and colonoscopy (Odd ratio: 4.84, 95% CI: 1.61-15.51; P = 0.0292; EGD as reference). It is noteworthy that ASA classification scores were not included as an independent predictive factor, and susceptibility of youth to hypoxemia during endoscopy was as high as old subjects. In conclusion, some certain pre-existing diseases of patients were newly identified as independent risk factors for hypoxemia during GI endoscopy. High ASA scores are a confounding predictive factor of pre-existing diseases. We thus recommend that youth (≤18 yrs), obese patients and those patients with hypertension, diabetes, heart diseases, or GI diseases should be monitored closely during sedation endoscopy.
低氧血症是胃肠道内镜检查中最常见的不良事件。为了在检查前估计低氧血症的风险,美国麻醉医师协会(ASA)分类评分被用作主要预测因素。但是,由于该分类系统忽略了许多可能导致低氧血症的一般健康状况和患者适应性的信息,因此人们对 ASA 评分预测低氧血症发生率的准确性产生了怀疑。在这项前瞻性收集的临床数据回顾性分析中,分析了 4904 例手术的数据。使用 Pearson's chi-square 检验或 Fisher 确切检验分析分类因素的方差。连续变量使用 t 检验或方差分析(ANOVA)进行统计学评估。结果,在纳入的 4904 例患者中,仅发现 245 例(5.0%)在检查过程中出现低氧血症。多变量逻辑回归显示,低氧血症的独立危险因素包括高 BMI(BMI 30 与 20,比值比:1.52,95%CI:1.13-2.05;P=0.0098)、高血压(比值比:2.28,95%CI:1.44-3.60;P=0.0004)、糖尿病(比值比:2.37,95%CI:1.30-4.34;P=0.005)、胃肠道疾病(比值比:1.77,95%CI:1.21-2.60;P=0.0033)、心脏病(比值比:1.97,95%CI:1.06-3.68;P=0.0325)和联合食管胃十二指肠镜检查(EGD)和结肠镜检查的程序(比值比:4.84,95%CI:1.61-15.51;P=0.0292;以 EGD 为参考)。值得注意的是,ASA 分类评分未被纳入独立预测因素,并且年轻人在检查过程中发生低氧血症的易感性与老年患者一样高。总之,一些患者的某些预先存在的疾病被新确定为胃肠道内镜检查期间低氧血症的独立危险因素。高 ASA 评分是预先存在疾病的混杂预测因素。因此,我们建议对青年(≤18 岁)、肥胖患者以及患有高血压、糖尿病、心脏病或胃肠道疾病的患者,在镇静内镜检查期间应密切监测。