Chan Paul S, Spertus John A, Krumholz Harlan M, Berg Robert A, Li Yan, Sasson Comilla, Nallamothu Brahmajee K
Saint Luke's Mid America Heart Institute, Kansas City, Missouri 64111, USA.
Arch Intern Med. 2012 Jun 25;172(12):947-53. doi: 10.1001/archinternmed.2012.2050.
Accurate estimation of favorable neurological survival after in-hospital cardiac arrest could provide critical information for physicians, patients, and families.
Within the Get With the Guidelines-Resuscitation registry, we identified 42,957 patients from 551 hospitals admitted between January 2000 and October 2009 who were successfully resuscitated from an in-hospital cardiac arrest. A simple prediction tool for favorable neurological survival in patients successfully resuscitated from an in-hospital cardiac arrest was developed using multivariate logistic regression, with two-thirds of the sample randomly selected as the derivation cohort and one-third as the validation cohort. Favorable neurological status was defined as the absence of severe neurological deficits (cerebral performance category score of ≤2).
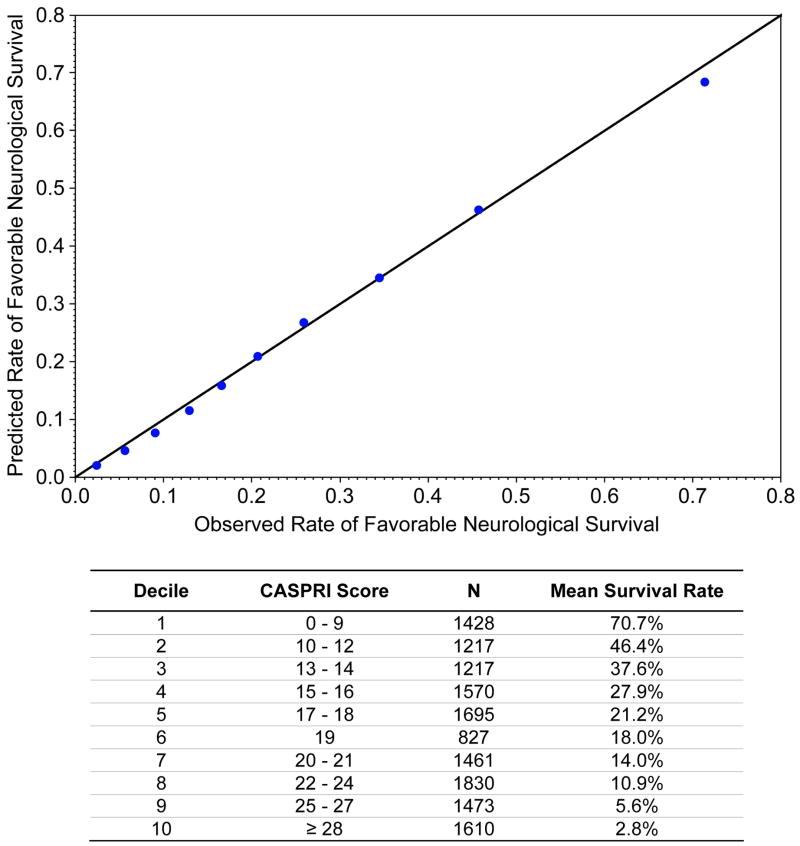
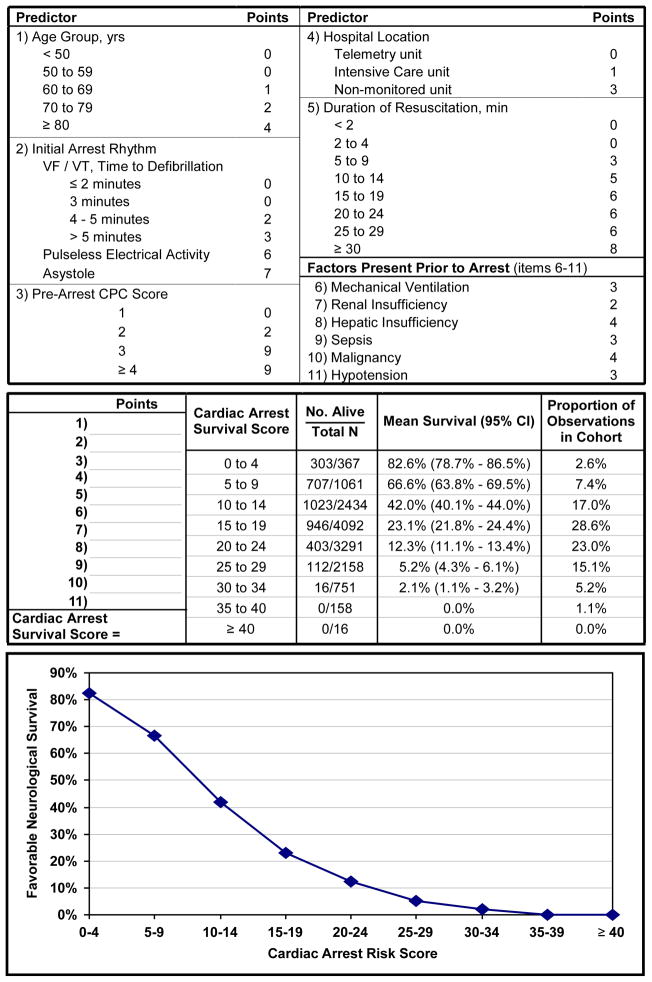
Rates of favorable neurological survival were similar in the derivation cohort (7052 patients [24.6%]) and validation cohort (3510 patients [24.5%]). Eleven variables were associated with favorable neurological survival: younger age, initial cardiac arrest rhythm of ventricular fibrillation or pulseless ventricular tachycardia with a defibrillation time of 2 minutes or less, baseline neurological status without disability, arrest location in a monitored unit, shorter duration of resuscitation, and absence of mechanical ventilation, renal insufficiency, hepatic insufficiency, sepsis, malignant disease, and hypotension prior to the arrest. The model had excellent discrimination (C statistic of 0.80 for both the derivation and validation cohorts) and calibration. The prediction tool demonstrated the ability to identify patients across a wide range of rates of favorable neurological survival: patients in the top decile had a 70.7% probability of this outcome, whereas patients in the bottom decile had a 2.8% probability.
Among successfully resuscitated patients with an in-hospital cardiac arrest, a simple, bedside prediction tool provides robust estimates of the probability of favorable neurological survival. This tool permits accurate prognostication after cardiac arrest for physicians, patients, and families.
准确估计院内心脏骤停后良好神经功能存活情况可为医生、患者及其家属提供关键信息。
在“遵循复苏指南”注册研究中,我们从551家医院中确定了2000年1月至2009年10月期间收治的42957例院内心脏骤停后成功复苏的患者。使用多变量逻辑回归开发了一种用于预测院内心脏骤停后成功复苏患者良好神经功能存活情况的简单预测工具,将三分之二的样本随机选为推导队列,三分之一作为验证队列。良好神经功能状态定义为无严重神经功能缺损(脑功能分类评分≤2)。
推导队列(7052例患者[24.6%])和验证队列(3510例患者[24.5%])中良好神经功能存活的发生率相似。11个变量与良好神经功能存活相关:年龄较小、初始心脏骤停节律为室颤或无脉性室速且除颤时间在2分钟或更短、基线神经功能状态无残疾、在监测病房发生骤停、复苏持续时间较短,以及在骤停前无机械通气、肾功能不全、肝功能不全、脓毒症、恶性疾病和低血压。该模型具有出色的辨别力(推导队列和验证队列的C统计量均为0.80)和校准度。该预测工具显示能够识别不同良好神经功能存活发生率范围内的患者:处于最高十分位数的患者出现这种结果的概率为70.7%,而处于最低十分位数的患者概率为2.8%。
在院内心脏骤停后成功复苏的患者中,一种简单的床边预测工具可对良好神经功能存活的概率提供可靠估计。该工具可为医生、患者及其家属在心脏骤停后进行准确的预后判断。