Departments of Psychiatry and Pediatrics, The University of Iowa Carver College of Medicine, 500 Newton Road, Iowa City, IA 52242, USA.
Child Adolesc Psychiatry Ment Health. 2012 May 29;6(1):21. doi: 10.1186/1753-2000-6-21.
Most clinical trials of antipsychotics in children are brief, failing to address their long-term safety, particularly when taken concurrently with other psychotropics. This hypothesis-generating analysis evaluates potential correlates of weight gain in children receiving extended risperidone treatment.
Medically healthy 7-17 year-old patients treated with risperidone for six months or more were enrolled. Anthropometric measurements were conducted. Developmental and medication history was obtained from the medical record. Information related to birth weight, dietary intake, physical activity, and parental weight was collected. Mixed regression analyses explored the contribution of various demographic and clinical factors to age- and sex-adjusted weight and body mass index (BMI) z scores over the treatment period.
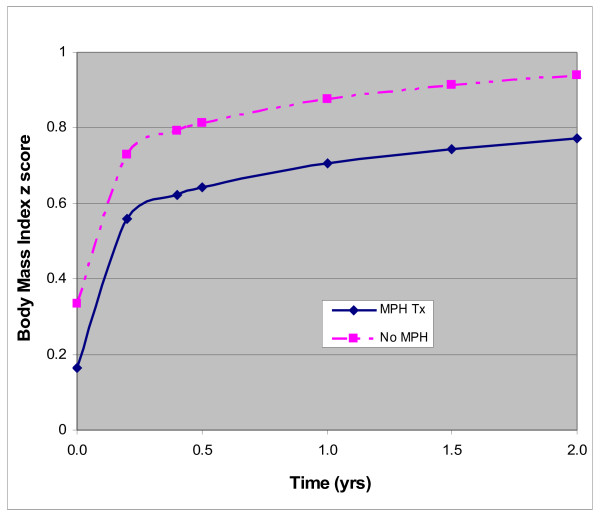
The sample consisted of 110 patients (89% males) with a mean age of 11.8 years (sd = 2.9) upon enrollment. The majority had an externalizing disorder and received 0.03 mg/kg/day (sd = 0.02) of risperidone, for 2.5 years (sd = 1.7), to primarily target irritability and aggression (81%). Polypharmacy was common with 71% receiving psychostimulants, 50% selective serotonin reuptake inhibitors (SSRIs), and 32% α2-agonists. Weight and BMI z score were positively correlated with baseline weight at the start of risperidone, treatment duration, and the weight-adjusted dose of risperidone but inversely associated with the weight-adjusted dose of psychostimulants and the concurrent use of SSRIs and α2-agonists. The effect of risperidone dose appeared to attenuate as treatment extended while that of psychostimulants became more significant. The rate of change in weight (or BMI) z score prior to and within the first 12 weeks of risperidone treatment did not independently predict future changes neither did birth weight, postnatal growth, dietary intake, physical activity, or parental weight.
This comprehensive analysis exploring correlates of long-term weight (or BMI) change in risperidone-treated youths revealed that pharmacotherapy exerts significant but complex effects.
Not applicable.
大多数儿童抗精神病药物的临床试验时间都很短,无法解决其长期安全性问题,尤其是当与其他精神药物同时使用时。本假说生成分析评估了接受延长利培酮治疗的儿童体重增加的潜在相关因素。
纳入接受利培酮治疗六个月或更长时间的 7-17 岁健康儿童患者。进行人体测量学测量。从病历中获得发育和用药史。收集与出生体重、饮食摄入、体力活动和父母体重相关的信息。混合回归分析探讨了各种人口统计学和临床因素对治疗期间年龄和性别调整后的体重和体重指数(BMI)z 评分的贡献。
样本包括 110 名患者(89%为男性),入组时平均年龄为 11.8 岁(标准差=2.9)。大多数患者患有外在障碍,接受 0.03mg/kg/天(标准差=0.02)的利培酮治疗,为期 2.5 年(标准差=1.7),主要针对易激惹和攻击行为(81%)。联合用药很常见,71%的患者接受了精神兴奋剂,50%接受了选择性 5-羟色胺再摄取抑制剂(SSRIs),32%接受了α2-激动剂。体重和 BMI z 评分与利培酮开始时的基线体重、治疗持续时间和利培酮的体重调整剂量呈正相关,与精神兴奋剂的体重调整剂量以及同时使用 SSRIs 和 α2-激动剂呈负相关。利培酮剂量的影响似乎随着治疗的延长而减弱,而精神兴奋剂的影响则变得更加显著。利培酮治疗前和前 12 周内体重(或 BMI)z 评分的变化率不能独立预测未来的变化,出生体重、产后生长、饮食摄入、体力活动或父母体重也不能预测。
这项探索利培酮治疗青少年长期体重(或 BMI)变化相关因素的综合分析表明,药物治疗具有显著但复杂的影响。
不适用。