Department of Practice and Policy, UCL School of Pharmacy, BMA House, Mezzanine Floor, Tavistock Square, London, WC1H 9JP, UK.
BMC Health Serv Res. 2012 Jun 10;12:150. doi: 10.1186/1472-6963-12-150.
Failure Mode and Effects Analysis (FMEA) is a prospective risk assessment tool that has been widely used within the aerospace and automotive industries and has been utilised within healthcare since the early 1990s. The aim of this study was to explore the validity of FMEA outputs within a hospital setting in the United Kingdom.
Two multidisciplinary teams each conducted an FMEA for the use of vancomycin and gentamicin. Four different validity tests were conducted: Face validity: by comparing the FMEA participants' mapped processes with observational work. Content validity: by presenting the FMEA findings to other healthcare professionals. Criterion validity: by comparing the FMEA findings with data reported on the trust's incident report database. Construct validity: by exploring the relevant mathematical theories involved in calculating the FMEA risk priority number.
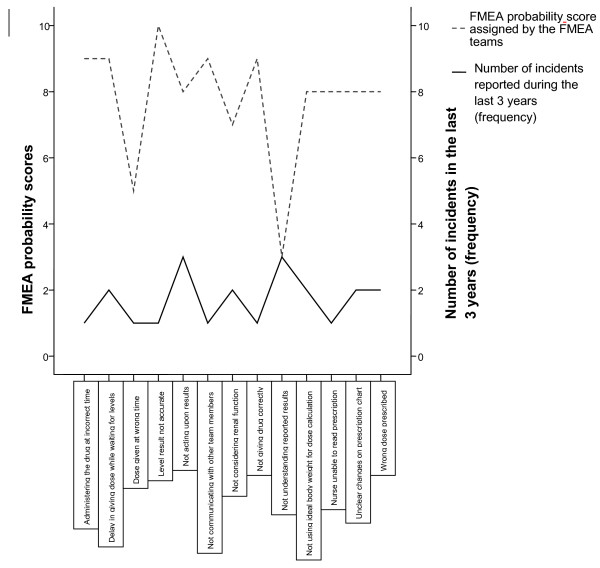
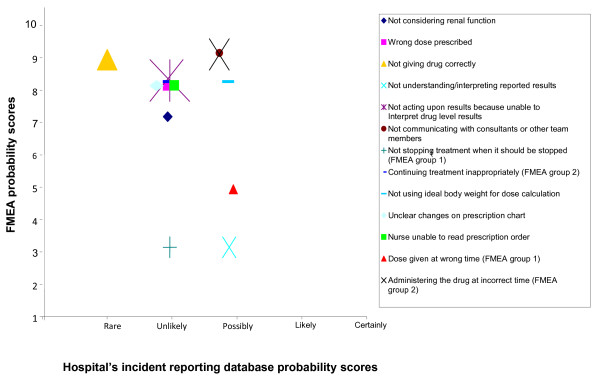
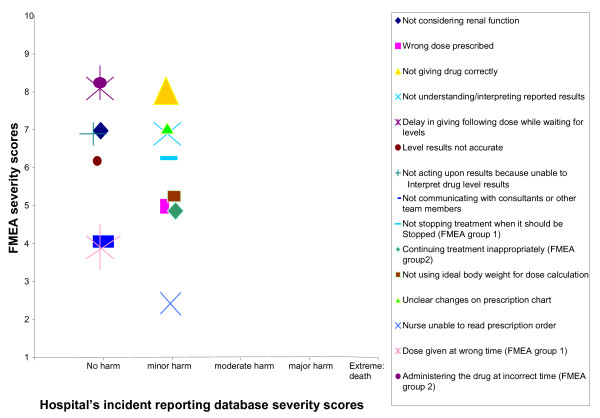
Face validity was positive as the researcher documented the same processes of care as mapped by the FMEA participants. However, other healthcare professionals identified potential failures missed by the FMEA teams. Furthermore, the FMEA groups failed to include failures related to omitted doses; yet these were the failures most commonly reported in the trust's incident database. Calculating the RPN by multiplying severity, probability and detectability scores was deemed invalid because it is based on calculations that breach the mathematical properties of the scales used.
There are significant methodological challenges in validating FMEA. It is a useful tool to aid multidisciplinary groups in mapping and understanding a process of care; however, the results of our study cast doubt on its validity. FMEA teams are likely to need different sources of information, besides their personal experience and knowledge, to identify potential failures. As for FMEA's methodology for scoring failures, there were discrepancies between the teams' estimates and similar incidents reported on the trust's incident database. Furthermore, the concept of multiplying ordinal scales to prioritise failures is mathematically flawed. Until FMEA's validity is further explored, healthcare organisations should not solely depend on their FMEA results to prioritise patient safety issues.
失效模式与影响分析(FMEA)是一种前瞻性风险评估工具,已在航空航天和汽车行业得到广泛应用,并自 20 世纪 90 年代初以来在医疗保健领域得到应用。本研究的目的是探讨 FMEA 在英国医院环境中的有效性。
两个多学科团队分别对万古霉素和庆大霉素的使用进行了 FMEA。进行了四项不同的有效性测试:
表面有效性:通过比较 FMEA 参与者绘制的流程与观察性工作。
内容有效性:通过向其他医疗保健专业人员展示 FMEA 结果。
标准有效性:通过将 FMEA 结果与信托的事件报告数据库中报告的数据进行比较。
构建有效性:通过探索计算 FMEA 风险优先数所涉及的相关数学理论。
表面有效性是积极的,因为研究人员记录了与 FMEA 参与者绘制的相同的护理过程。然而,其他医疗保健专业人员发现了 FMEA 团队遗漏的潜在故障。此外,FMEA 小组未能包括与遗漏剂量相关的故障;然而,这些是信托事件数据库中最常报告的故障。通过将严重程度、概率和可检测性得分相乘来计算 RPN 被认为是无效的,因为它基于违反使用的量表的数学特性的计算。
验证 FMEA 存在重大的方法学挑战。它是帮助多学科团队绘制和理解护理过程的有用工具;然而,我们的研究结果对其有效性提出了质疑。FMEA 团队可能需要除个人经验和知识之外的其他信息来源来识别潜在的故障。至于 FMEA 用于对故障进行评分的方法,团队的估计与信托事件数据库中报告的类似事件之间存在差异。此外,将有序量表相乘以对故障进行优先级排序的概念在数学上是有缺陷的。在进一步探索 FMEA 的有效性之前,医疗保健组织不应该仅仅依靠他们的 FMEA 结果来确定患者安全问题的优先级。