Division of Metabolism, Endocrinology, and Diabetes, Department of Medicine, University of Michigan, Ann Arbor, Michigan 48109, USA.
Cancer. 2013 Jan 15;119(2):259-65. doi: 10.1002/cncr.27721. Epub 2012 Jun 28.
There is controversy regarding the optimal management of thyroid cancer. The proportion of patients with low-risk thyroid cancer who received radioactive iodine (RAI) treatment increased over the last 20 years, and little is known about the role played by clinicians in hospital-level RAI use for low-risk disease.
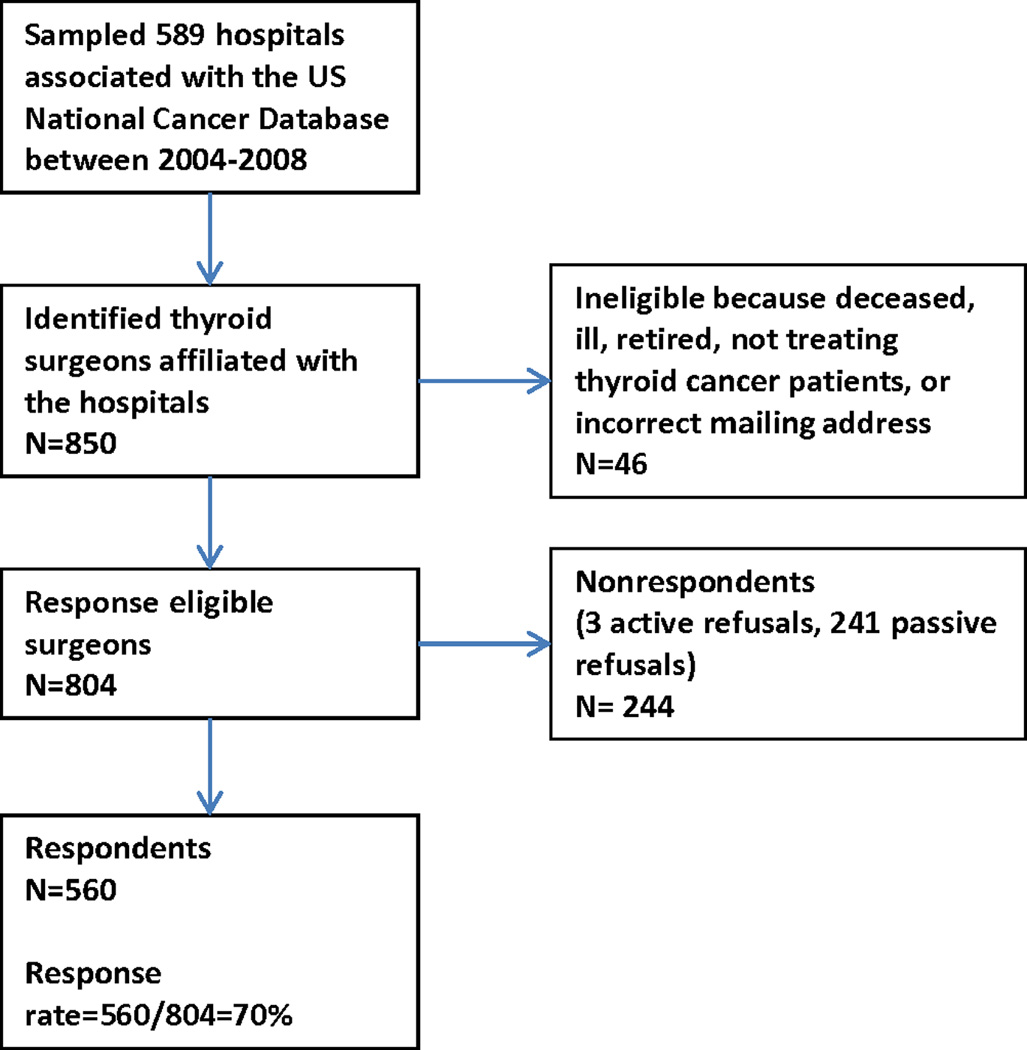
Thyroid surgeons affiliated with 368 hospitals that had Commission on Cancer-accredited cancer programs were surveyed. Survey data were linked to data reported to the National Cancer Database. A multivariable analysis was used to assess the relation between clinician decision makers and hospital-level RAI use after total thyroidectomy in patients with stage I, well differentiated thyroid cancer.
The survey response rate was 70% (560 of 804 surgeons). The surgeon was identified as the primary decision maker by 16% of the surgeons; the endocrinologist was identified as the primary decision maker by 69%, and a nuclear medicine, radiologist, or other physician was identified as the primary decision maker by 15%. In a multivariable analysis controlling for hospital case volume and hospital type, when the primary decision maker was in a specialty other than endocrinology or surgery, there was greater use of RAI at the hospital (P < .001). A greater number of providers at the hospital where RAI was administered and having access to a tumor board also were associated with increased use of RAI (P < .001 and P = .006, respectively).
The specialty of the primary decision maker, the number of providers administering RAI, and having access to a tumor board were associated significantly with the use of RAI for stage I thyroid cancer. The findings have implications for addressing nonclinical variation between hospitals, with a marked heterogeneity in decision making suggesting that standardization of care will be challenging.
甲状腺癌的最佳治疗方案存在争议。在过去的 20 年中,接受放射性碘(RAI)治疗的低危甲状腺癌患者比例有所增加,但对于临床医生在医院层面上对低危疾病使用 RAI 的作用知之甚少。
对 368 家拥有癌症委员会认证癌症项目的甲状腺外科医生进行了调查。调查数据与国家癌症数据库报告的数据相关联。使用多变量分析评估了在 I 期分化良好的甲状腺癌患者中,甲状腺外科医生和内分泌医生作为决策者与全甲状腺切除术后医院层面 RAI 使用之间的关系。
调查的回复率为 70%(804 名外科医生中的 560 名)。16%的外科医生认为外科医生是主要决策者;69%的医生认为内分泌医生是主要决策者,15%的医生认为核医学、放射科医生或其他医生是主要决策者。在控制医院病例量和医院类型的多变量分析中,当主要决策者是内分泌科或外科以外的专业人员时,医院使用 RAI 的比例更高(P<0.001)。在医院中实施 RAI 的医生数量更多,并且能够获得肿瘤委员会的支持,也与 RAI 使用的增加相关(P<0.001 和 P=0.006)。
主要决策者的专业、实施 RAI 的医生数量以及获得肿瘤委员会的支持与 I 期甲状腺癌使用 RAI 显著相关。这些发现对解决医院间非临床差异具有重要意义,决策的明显异质性表明标准化护理将具有挑战性。