King Faisal Hospital, Kigali, Rwanda.
PLoS One. 2012;7(6):e31572. doi: 10.1371/journal.pone.0031572. Epub 2012 Jun 26.
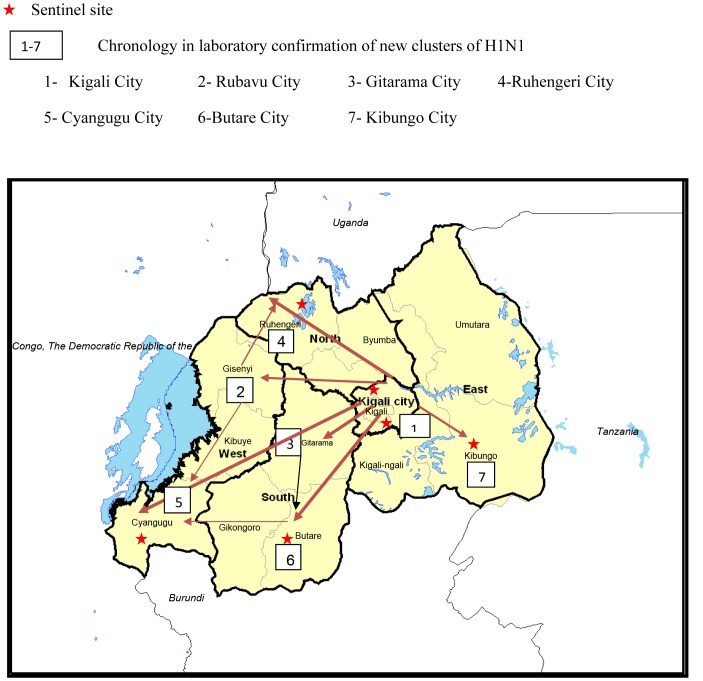
In October 2009, the first case of pandemic influenza A(H1N1)pdm09 (pH1N1) was confirmed in Kigali, Rwanda and countrywide dissemination occurred within several weeks. We describe clinical and epidemiological characteristics of this epidemic.
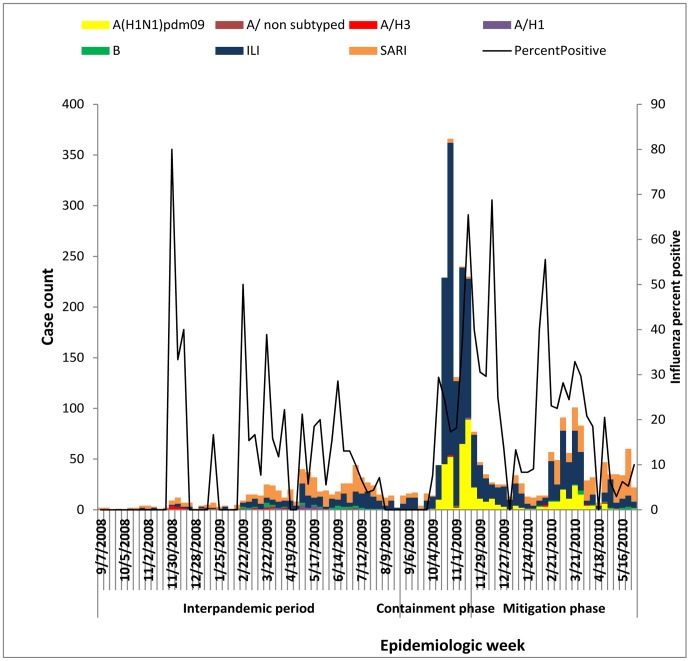
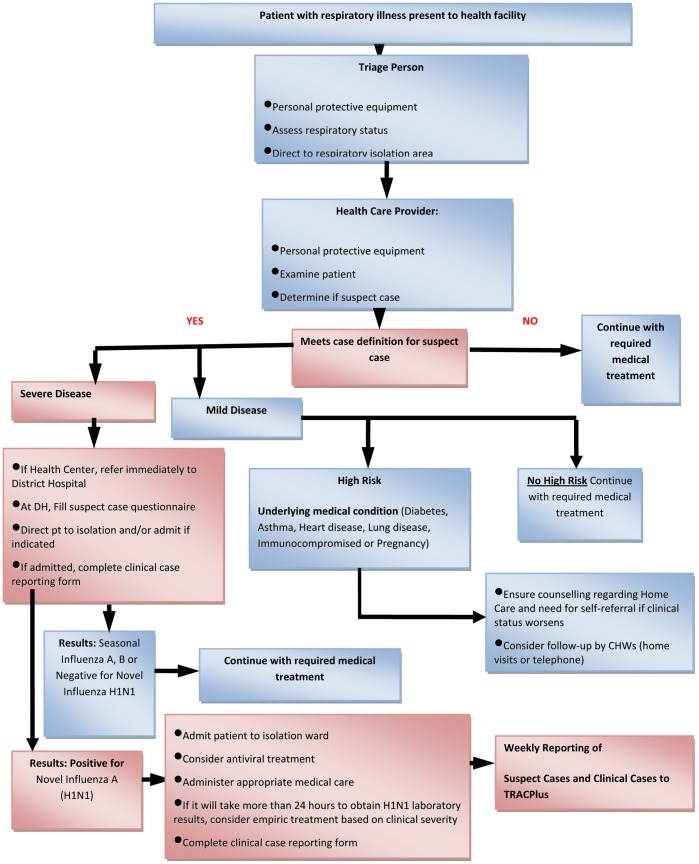
From October 2009 through May 2010, we undertook epidemiologic investigations and response to pH1N1. Respiratory specimens were collected from all patients meeting the WHO case definition for pH1N1, which were tested using CDC's real time RT-PCR protocol at the Rwandan National Reference Laboratory (NRL). Following documented viral transmission in the community, testing focused on clinically severe and high-risk group suspect cases.
From October 9, 2009 through May 31, 2010, NRL tested 2,045 specimens. In total, 26% (n = 532) of specimens tested influenza positive; of these 96% (n = 510) were influenza A and 4% (n = 22) were influenza B. Of cases testing influenza A positive, 96.8% (n = 494), 3% (n = 15), and 0.2% (n = 1) were A(H1N1)pdm09, Seasonal A(H3) and Seasonal A(non-subtyped), respectively. Among laboratory-confirmed cases, 263 (53.2%) were children <15 years and 275 (52%) were female. In total, 58 (12%) cases were hospitalized with mean duration of hospitalization of 5 days (Range: 2-15 days). All cases recovered and there were no deaths. Overall, 339 (68%) confirmed cases received oseltamivir in any setting. Among all positive cases, 26.9% (143/532) were among groups known to be at high risk of influenza-associated complications, including age <5 years 23% (122/532), asthma 0.8% (4/532), cardiac disease 1.5% (8/532), pregnancy 0.6% (3/532), diabetes mellitus 0.4% (2/532), and chronic malnutrition 0.8% (4/532).
Rwanda experienced a PH1N1 outbreak which was epidemiologically similar to PH1N1 outbreaks in the region. Unlike seasonal influenza, children <15 years were the most affected by pH1N1. Lessons learned from the outbreak response included the need to strengthen integrated disease surveillance, develop laboratory contingency plans, and evaluate the influenza sentinel surveillance system.
2009 年 10 月,首例大流行流感 A(H1N1)pdm09(pH1N1)在卢旺达基加利被确认,数周内便在全国范围内传播。我们描述了此次疫情的临床和流行病学特征。
从 2009 年 10 月至 2010 年 5 月,我们对 pH1N1 进行了流行病学调查和应对。所有符合世卫组织 pH1N1 病例定义的患者都采集了呼吸道标本,并在卢旺达国家参考实验室(NRL)使用疾控中心的实时 RT-PCR 方案进行检测。在社区内有记录的病毒传播后,检测重点放在临床严重和高风险组疑似病例上。
从 2009 年 10 月 9 日至 2010 年 5 月 31 日,NRL 共检测了 2045 份标本。总共,26%(n=532)的标本流感检测呈阳性;其中 96%(n=510)为甲型流感,4%(n=22)为乙型流感。甲型流感阳性病例中,96.8%(n=494)、3%(n=15)和 0.2%(n=1)分别为 A(H1N1)pdm09、季节性 A(H3)和季节性 A(未分型)。在实验室确诊的病例中,263 例(53.2%)为<15 岁的儿童,275 例(52%)为女性。总共,58 例(12%)住院,平均住院时间为 5 天(范围:2-15 天)。所有病例均康复,无死亡。总体而言,339 例(68%)确诊病例在任何环境中都接受了奥司他韦治疗。在所有阳性病例中,26.9%(143/532)属于已知有流感相关并发症高风险的人群,包括年龄<5 岁者 23%(122/532)、哮喘 0.8%(4/532)、心脏病 1.5%(8/532)、妊娠 0.6%(3/532)、糖尿病 0.4%(2/532)和慢性营养不良 0.8%(4/532)。
卢旺达发生了一起与该地区 pH1N1 暴发类似的大流行流感 A(H1N1)pdm09 暴发。与季节性流感不同,<15 岁的儿童是受 pH1N1 影响最严重的人群。疫情应对中吸取的经验教训包括需要加强综合疾病监测、制定实验室应急计划和评估流感哨点监测系统。