Department of Surgery, Washington University School of Medicine, St. Louis, MO, USA.
Cytokine. 2012 Oct;60(1):249-56. doi: 10.1016/j.cyto.2012.06.016. Epub 2012 Jun 28.
Management of sepsis in critically ill patients remains difficult and requires prolonged intensive care. Genetic testing has been proposed as a strategy to identify patients at risk for adverse outcome of critical illnesses. Therefore, we wished to determine the influence of heredity on predisposition to poor outcome and on duration of ventilator support of intensive care unit (ICU) patients.
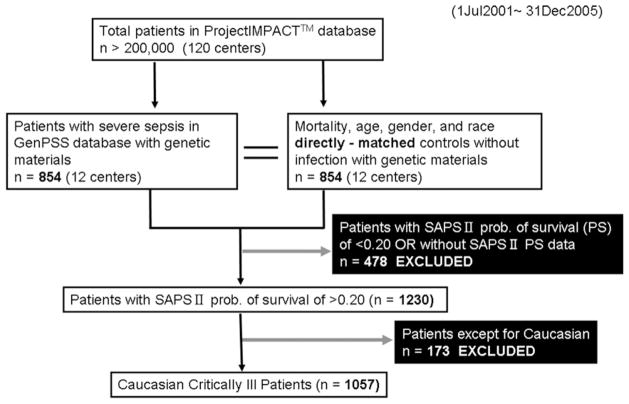
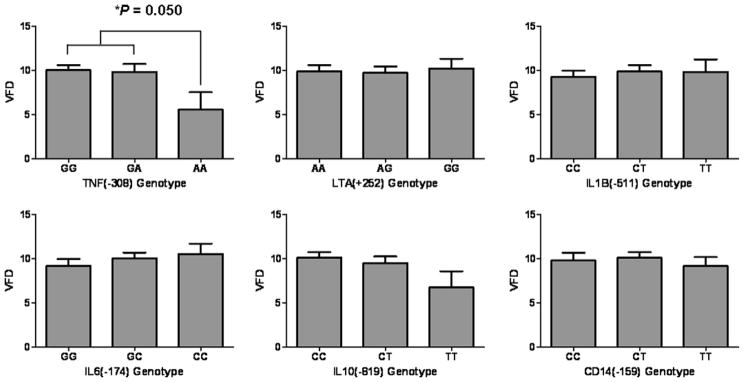
A study was conducted from July 2001 to December 2005 in heterogeneous population of patients from 12 US ICUs represented by the Genetic Predisposition to Severe Sepsis (GenPSS) archive. In 1057 Caucasian critically ill patients with SAPS II probability of survival of >0.2 in the US, six functional single nucleotide polymorphisms in relation to inflammatory cytokines and innate immunity (rs1800629, rs16944, rs1800795, rs1800871, rs2569190, and rs909253) were evaluated in terms of mortality and ventilator free days.
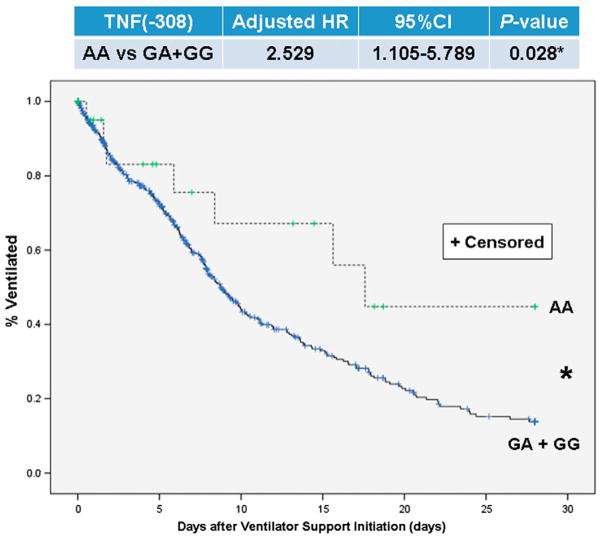
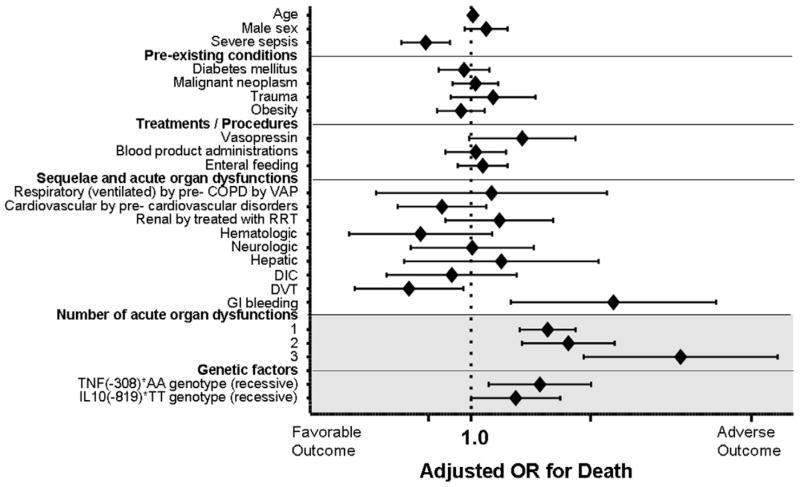
The AA homozygote of TNF(-308) (rs1800629) was most over-represented in the deceased patient group (P=0.015 with recessive model). The carriage of the TNF(-308)*AA genotype showed significantly higher odds ratio of 2.67(1.29-5.55) (P=0.008) after adjustment with the covariates. However, the presence of 1, 2, or 3 acute organ dysfunctions was larger prognostic factors for the adverse outcome (OR(95%CI)=2.98(2.00-4.45), 4.01(2.07-7.77), or 19.95(4.99-79.72), P<0.001 for all). Kaplan-Mayer plot on ventilator duration of TNF(-308)AA patient significantly diverged from that of TNF(-308)(GG+GA) ((AA v GG+GA), Adjusted HR(95%CI)=2.53(1.11-5.79) with Cox regression, P=0.028).
TNF(-308)*AA is significantly associated with susceptibility to adverse outcome and to longer ventilator duration. Therefore, heredity likely affects both predisposition to ICU prognosis as well as the resource utilization.
脓毒症患者的治疗仍然具有挑战性,需要长期的重症监护。基因检测已被提议作为一种策略,以确定患有危重病不良预后的患者。因此,我们希望确定遗传对不良预后和重症监护病房(ICU)患者呼吸机支持时间的影响。
这项研究于 2001 年 7 月至 2005 年 12 月在 12 个美国 ICU 的异质患者人群中进行,该人群由遗传易感性严重脓毒症(GenPSS)档案代表。在 1057 名白人危重病患者中,SAPS II 预测的存活率在美国>0.2,评估了与炎症细胞因子和固有免疫相关的六个功能性单核苷酸多态性(rs1800629、rs16944、rs1800795、rs1800871、rs2569190 和 rs909253),评估其死亡率和无呼吸机天数。
TNF(-308)(rs1800629)的 AA 纯合子在死亡患者组中最为常见(隐性模型,P=0.015)。携带 TNF(-308)*AA 基因型的患者的比值比明显更高,为 2.67(1.29-5.55)(P=0.008),经协变量调整后。然而,1、2 或 3 个急性器官功能障碍的存在是不良预后的更大预后因素(OR(95%CI)=2.98(2.00-4.45),4.01(2.07-7.77),或 19.95(4.99-79.72),P<0.001)。TNF(-308)AA 患者的呼吸机持续时间 Kaplan-Meier 图明显与 TNF(-308)(GG+GA)的呼吸机持续时间图不同((AA v GG+GA),Cox 回归的调整 HR(95%CI)=2.53(1.11-5.79),P=0.028)。
TNF(-308)*AA 与不良预后和更长的呼吸机时间显著相关。因此,遗传可能同时影响 ICU 预后和资源利用。