Department of Radiation Oncology, Mount Sinai Medical Center, New York, New York, United States of America.
PLoS One. 2012;7(6):e36979. doi: 10.1371/journal.pone.0036979. Epub 2012 Jun 27.
Preclinical data suggest that sunitinib enhances the efficacy of radiotherapy. We tested the combination of sunitinib and hypofractionated image-guided radiotherapy (IGRT) in a cohort of patients with historically incurable distant metastases.
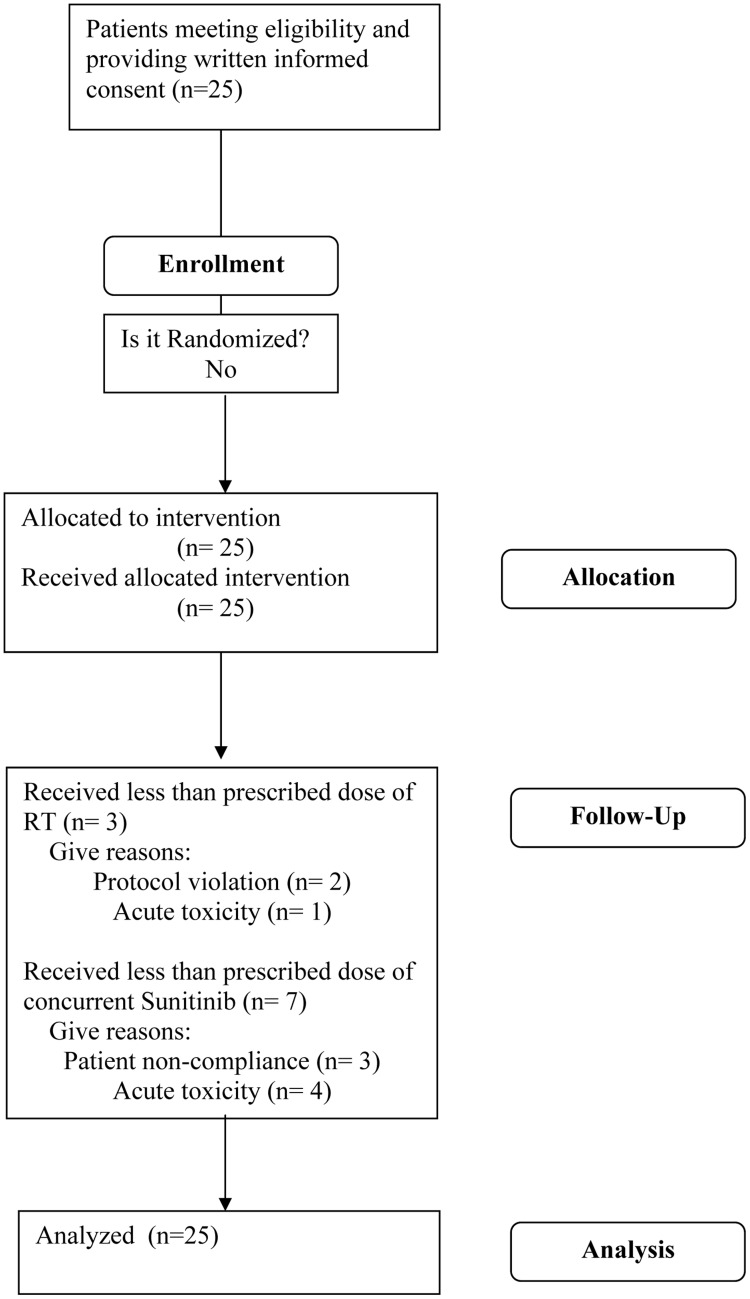
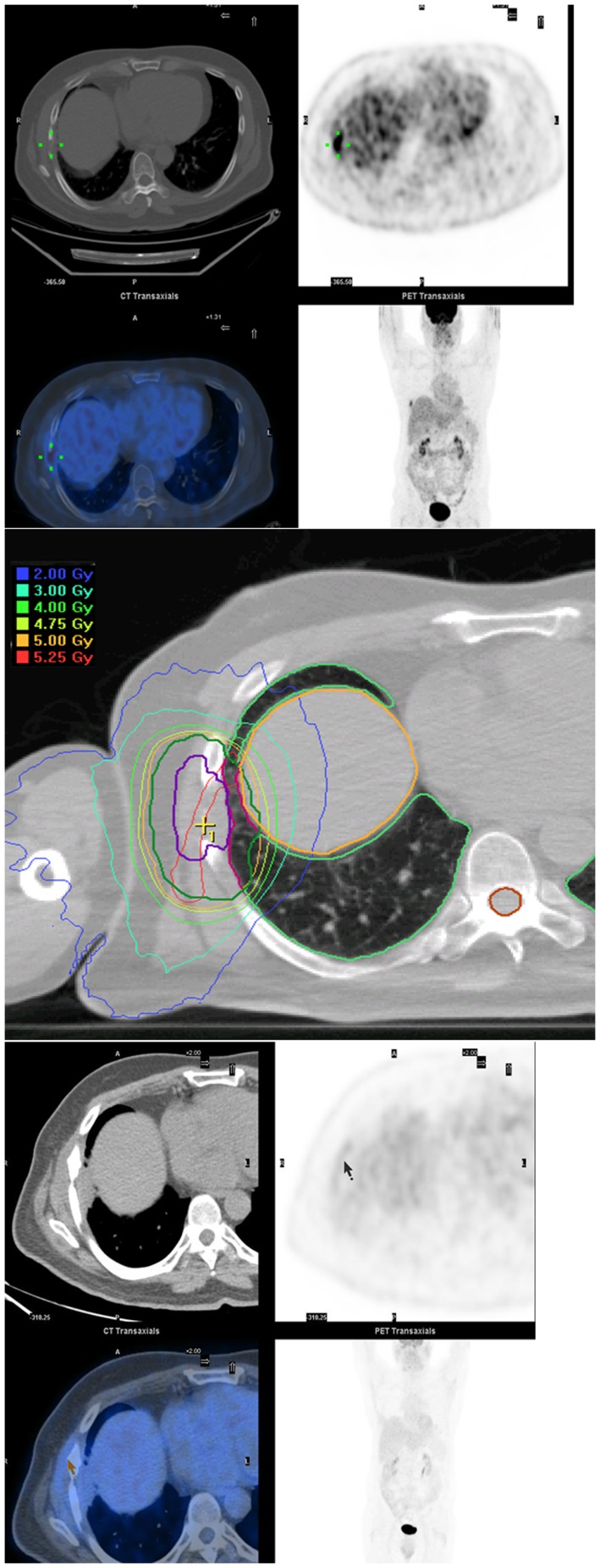
Twenty five patients with oligometastases, defined as 1-5 sites of active disease on whole body imaging, were enrolled in a phase II trial from 2/08 to 9/10. The most common tumor types treated were head and neck, liver, lung, kidney and prostate cancers. Patients were treated with the recommended phase II dose of 37.5 mg daily sunitinib (days 1-28) and IGRT 50 Gy (days 8-12 and 15-19). Maintenance sunitinib was used in 33% of patients. Median follow up was 17.5 months (range, 0.7 to 37.4 months).
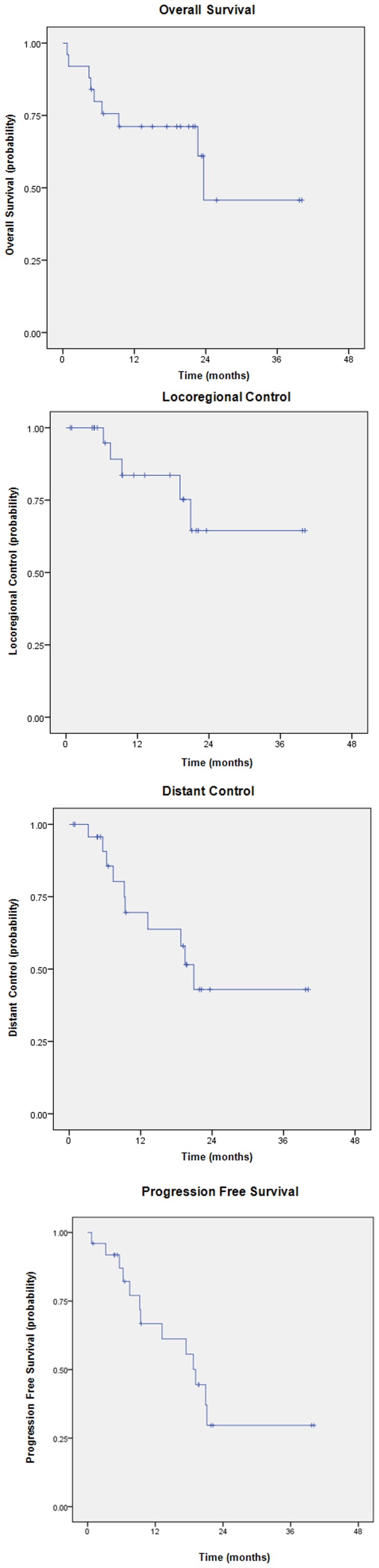
The 18-month local control, distant control, progression-free survival (PFS) and overall survival (OS) were 75%, 52%, 56% and 71%, respectively. At last follow-up, 11 (44%) patients were alive without evidence of disease, 7 (28%) were alive with distant metastases, 3 (12%) were dead from distant metastases, 3 (12%) were dead from comorbid illness, and 1 (4%) was dead from treatment-related toxicities. The incidence of acute grade ≥ 3 toxicities was 28%, most commonly myelosuppression, bleeding and abnormal liver function tests.
Concurrent sunitinib and IGRT achieves major clinical responses in a subset of patients with oligometastases.
ClinicalTrials.gov NCT00463060.
临床前数据表明舒尼替尼可增强放射治疗的疗效。我们在一组既往无法治愈的远处转移的患者中测试了舒尼替尼和适形分割图像引导放疗(IGRT)的联合应用。
从 2008 年 2 月至 2010 年 9 月,25 例寡转移患者(全身影像学检查有 1-5 个活动病灶)参加了这项 2 期临床试验。治疗的最常见肿瘤类型为头颈部、肝、肺、肾和前列腺癌。患者接受舒尼替尼推荐的 2 期剂量 37.5mg/d(第 1-28 天)和 IGRT 50Gy(第 8-12 天和第 15-19 天)。33%的患者接受维持性舒尼替尼治疗。中位随访时间为 17.5 个月(范围,0.7-37.4 个月)。
18 个月的局部控制、远处控制、无进展生存期(PFS)和总生存期(OS)分别为 75%、52%、56%和 71%。末次随访时,11 例(44%)患者无疾病存活,7 例(28%)患者有远处转移存活,3 例(12%)患者死于远处转移,3 例(12%)患者死于合并疾病,1 例(4%)患者死于治疗相关毒性。急性≥3 级毒性的发生率为 28%,最常见的是骨髓抑制、出血和肝功能异常。
在寡转移患者亚组中,舒尼替尼联合 IGRT 可获得主要的临床反应。
ClinicalTrials.gov NCT00463060。