Gürbüz Fatih, Kotan L Damla, Mengen Eda, Şıklar Zeynep, Berberoğlu Merih, Dökmetaş Sebila, Kılıçlı Mehmet Fatih, Güven Ayla, Kirel Birgül, Saka Nurçin, Poyrazoğlu Şükran, Cesur Yaşar, Doğan Murat, Özen Samim, Özbek Mehmet Nuri, Demirbilek Hüseyin, Kekil M Burcu, Temiz Fatih, Önenli Mungan Neslihan, Yüksel Bilgin, Topaloğlu Ali Kemal
Çukurova University Faculty of Medicine, Department of Pediatric Endocrinology, Balcalı, Adana, Turkey.
J Clin Res Pediatr Endocrinol. 2012 Sep;4(3):121-6. doi: 10.4274/jcrpe.725. Epub 2012 Jul 5.
Normosmic idiopathic hypogonadotropic hypogonadism (nIHH) is characterized by failure of initiation or maintenance of puberty due to insufficient gonadotropin release, which is not associated with anosmia/hyposmia. The objective of this study was to determine the distribution of causative mutations in a hereditary form of nIHH.
In this prospective collaborative study, 22 families with more than one affected individual (i.e. multiplex families) with nIHH were recruited and screened for genes known or suspected to be strong candidates for nIHH.
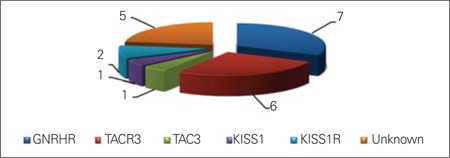
Mutations were identified in five genes (GNRHR, TACR3, TAC3, KISS1R, and KISS1) in 77% of families with autosomal recessively inherited nIHH. GNRHR and TACR3 mutations were the most common two causative mutations occurring with about equal frequency.
Mutations in these five genes account for about three quarters of the causative mutations in nIHH families with more than one affected individual. This frequency is significantly greater than the previously reported rates in all inclusive (familial plus sporadic) cohorts. GNRHR and TACR3 should be the first two genes to be screened for diagnostic purposes. Identification of causative mutations in the remaining families will shed light on the regulation of puberty.
嗅觉正常的特发性低促性腺激素性性腺功能减退症(nIHH)的特征是由于促性腺激素释放不足导致青春期启动或维持失败,且与嗅觉缺失/嗅觉减退无关。本研究的目的是确定遗传性nIHH中致病突变的分布情况。
在这项前瞻性合作研究中,招募了22个有不止一名nIHH患者的家庭(即多位点家庭),并对已知或疑似为nIHH强候选基因进行筛查。
在77%的常染色体隐性遗传nIHH家庭中,五个基因(GNRHR、TACR3、TAC3、KISS1R和KISS1)中发现了突变。GNRHR和TACR3突变是最常见的两种致病突变,发生频率大致相等。
这五个基因中的突变约占不止一名患者的nIHH家庭致病突变的四分之三。该频率显著高于先前在所有类型(家族性加散发性)队列中报告的发生率。GNRHR和TACR3应作为诊断目的首先筛查的两个基因。确定其余家庭中的致病突变将有助于了解青春期的调节机制。