Global Health Economics and Outcomes Research, Shire Development LLC., 725 Chesterbrook Boulevard, Wayne, PA 19087, USA.
Pharmacoeconomics. 2012 Aug 1;30(8):e1-15. doi: 10.2165/11632920-000000000-00000.
Attention-deficit hyperactivity disorder (ADHD) is a common psychiatric disorder in childhood, affecting 3-7% of school-age children in the US and imposing substantial economic burden. Stimulants are considered first-line pharmacological treatment and are the most prescribed treatment for ADHD. However, approximately 30% of children with ADHD do not have an optimal response to a single stimulant and may require adjunctive therapy.
Our objective was to conduct a cost-effectiveness analysis (CEA) of adding a non-stimulant, guanfacine extended release (GXR), to stimulants versus maintaining existing stimulant monotherapy in the treatment of ADHD in children and adolescents with suboptimal response to stimulant monotherapy.
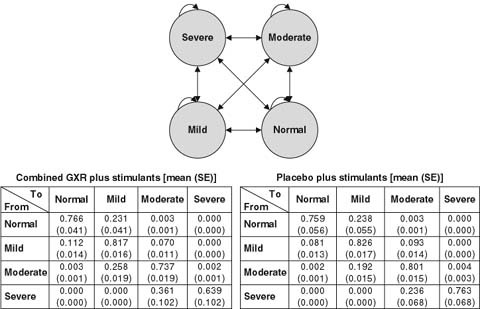
A 1-year Markov model was developed to estimate costs and effectiveness from a US third-party payer perspective. Effectiveness was measured by the QALY. The model assumed that patients transitioned among four health states (normal, mild, moderate and severe), defined by the Clinical Global Impression-Severity (CGI-S) scale. Transition probabilities were estimated in an ordered logit model using patient-level data from a multicentre, 9-week, double-blind, placebo-controlled, dose-optimization study, where subjects (n = 461) continued their stable morning stimulant and were randomized to GXR administered in the morning, GXR administered in the evening, or placebo. The model assumed that patients in moderate/severe health states after week 8 would discontinue ADHD treatment and remain in that state for the rest of the study period. Direct costs included drug wholesale acquisition costs and health state costs, all in $US, year 2010 values. Utility associated with each health state was obtained from the literature and disutilities associated with adverse events were applied for the first 4 weeks. One-way sensitivity analyses and probabilistic sensitivity analysis (PSA) were conducted by varying costs, utilities, adverse-event duration, and transition probabilities.
Compared with maintaining existing stimulant monotherapy, adding GXR to existing stimulant monotherapy was associated with an incremental drug cost of $US1016 but a lower medical cost of $US124, resulting in a total incremental cost of $US892 at 1 year. The addition of GXR to stimulants led to an incremental QALY of 0.03 and an incremental cost-effectiveness ratio (ICER) of $US31,660/QALY. In one-way sensitivity analysis, ICER values ranged from $US19,723, when 100% of patients were assumed to be severe in their initial health state, to $US46,631, when the last observed states from the clinical trial were carried forward to the end of the 1-year analysis period. PSA demonstrated a 94.6% likelihood that the ICER falls below $US50,000/QALY.
The impairment associated with residual ADHD symptoms after stimulant therapy is becoming increasingly recognized. This is the first analysis of the cost effectiveness of stimulants combined with an adjunctive medication. This study suggests that the adjunctive therapy of GXR with stimulants is a cost-effective treatment based on a willingness-to-pay threshold of $US50,000/QALY. This may address an unmet need among patients with suboptimal response to stimulant monotherapy.
注意缺陷多动障碍(ADHD)是儿童期常见的精神疾病,影响美国 3-7%的学龄儿童,并造成巨大的经济负担。兴奋剂被认为是一线药物治疗方法,也是 ADHD 最常开的治疗药物。然而,大约 30%的 ADHD 儿童对单一兴奋剂没有最佳反应,可能需要辅助治疗。
我们旨在针对对单一兴奋剂反应不佳的儿童和青少年 ADHD 患者,进行一项成本效益分析(CEA),即在维持现有兴奋剂单药治疗的基础上,添加非兴奋剂胍法辛缓释剂(GXR)的治疗方案与前者相比,哪一个更具成本效益。
我们建立了一个为期 1 年的 Markov 模型,以从美国第三方支付者的角度评估成本和效果。效果用 QALY 来衡量。模型假设患者在四个健康状态(正常、轻度、中度和重度)之间转移,由临床总体印象严重度量表(CGI-S)定义。使用多中心、9 周、双盲、安慰剂对照、剂量优化研究中的患者水平数据,在有序逻辑回归模型中估计转移概率,其中(n=461)患者继续稳定的早晨兴奋剂治疗,并随机分配到 GXR 早晨给药、GXR 晚上给药或安慰剂。模型假设第 8 周后处于中度/重度健康状态的患者将停止 ADHD 治疗,并在研究期间的剩余时间内保持该状态。直接成本包括药物批发采购成本和健康状态成本,均以 2010 年美元计价。从文献中获得与每个健康状态相关的效用,并在前 4 周应用与不良反应相关的不效用。通过改变成本、效用、不良反应持续时间和转移概率进行了单因素敏感性分析和概率敏感性分析(PSA)。
与维持现有兴奋剂单药治疗相比,在维持现有兴奋剂单药治疗的基础上添加 GXR 会增加 1016 美元的药物成本,但会降低 124 美元的医疗成本,因此 1 年的总增量成本为 892 美元。添加 GXR 可使兴奋剂治疗的增量 QALY 增加 0.03,增量成本效益比(ICER)为 31660 美元/QALY。在单因素敏感性分析中,ICER 值范围从当假设 100%的患者初始健康状态为重度时的 19723 美元,到当临床试验的最后观察状态延续到 1 年分析期结束时的 46631 美元。PSA 显示,ICER 低于 50000 美元/QALY 的可能性为 94.6%。
人们越来越认识到兴奋剂治疗后残留 ADHD 症状所带来的损害。这是第一项关于兴奋剂联合辅助药物的成本效益分析。这项研究表明,GXR 与兴奋剂联合辅助治疗是一种具有成本效益的治疗方法,基于 50000 美元/QALY 的意愿支付阈值。这可能满足了对兴奋剂单药治疗反应不佳的患者的未满足需求。




