Department of Medicine, Division of Hematology and Oncology, Advocate Lutheran General Hospital, Park Ridge, IL, USA.
Br J Cancer. 2012 Aug 7;107(4):592-7. doi: 10.1038/bjc.2012.312. Epub 2012 Jul 17.
Determining the maximum tolerated dose (MTD) and the dose-limiting toxicity (DLT) of sorafenib (S) plus imatinib (IM) in castration-resistant prostate cancer (CRPC) patients.
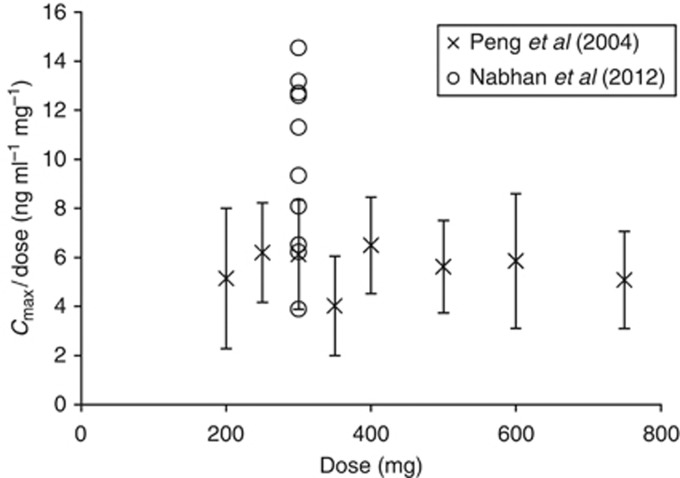
Refractory CRPC patients were enrolled onto this 3+3 dose escalation designed study. Imatinib pharmacokinetics (PK) were determined on day 15, 4 h post dose with a validated LC-MS assay.
Seventeen patients were enrolled; 10 evaluable (6 at 400 mg S qd with 300 mg IM qd (DL0) and 4 at 400 mg S bid with 300 mg IM qd (DL1)); inevaluable patients received <1 cycle. The median age was 73 (57-89); median prostatic serum antigen was 284 ng ml(-1) (11.7-9027). Median number of prior non-hormonal therapies was 3 (1-12). Dose-limiting toxicities were diarrhoea and hand-foot syndrome. Maximum tolerated dose was 400 mg S and 300 mg IM both daily. No biochemical responses were observed. Two patients had stable disease by RECIST. Median time to progression was 2 months (1-5). Median OS was 6 months (1-30+) with 3/17 patients (17%) alive at 21 months median follow-up. Ten patients had PK data suggesting that S reduced IM clearance by 55%, resulting in 77% increased exposure (P=0.005; compared with historical data).
This is the first report showing that S+IM can be administered in CRPC at a dose of 400 mg S and 300 mg IM, daily.
评估索拉非尼(S)联合伊马替尼(IM)在去势抵抗性前列腺癌(CRPC)患者中的最大耐受剂量(MTD)和剂量限制性毒性(DLT)。
这项 3+3 剂量递增设计的研究纳入了难治性 CRPC 患者。在第 15 天,给予伊马替尼后 4 小时,采用经验证的 LC-MS 检测法测定伊马替尼的药代动力学(PK)。
共纳入 17 例患者,10 例可评估(6 例接受 400 mg S 每日 1 次联合 300 mg IM 每日 1 次(DL0),4 例接受 400 mg S 每日 2 次联合 300 mg IM 每日 1 次(DL1));不可评估的患者接受了<1 个周期的治疗。患者中位年龄为 73 岁(57-89 岁);中位前列腺特异性抗原为 284ng/ml(11.7-9027)。中位既往非激素治疗次数为 3 次(1-12 次)。剂量限制性毒性为腹泻和手足综合征。最大耐受剂量为 400 mg S 和 300 mg IM 每日各 1 次。未观察到生化缓解。2 例患者根据 RECIST 标准评估为疾病稳定。中位无进展生存期为 2 个月(1-5 个月)。中位总生存期为 6 个月(1-30+),中位随访 21 个月时,3/17 例患者(17%)存活。10 例患者的 PK 数据表明,S 使 IM 清除率降低 55%,导致 IM 暴露增加 77%(P=0.005;与历史数据相比)。
这是首个报道表明,S+IM 可用于 CRPC 患者,剂量为 400 mg S 和 300 mg IM,每日各 1 次。