1st Division of Infectious Diseases, Luigi Sacco Hospital, Milano, Italy.
PLoS One. 2012;7(7):e39222. doi: 10.1371/journal.pone.0039222. Epub 2012 Jul 11.
Long term efficacy of raltegravir (RAL)-including regimens in highly pre-treated HIV-1-infected patients has been demonstrated in registration trials. However, few studies have assessed durability in routine clinical settings.
Antiretroviral treatment-experienced patients initiating a RAL-containing salvage regimen were enrolled. Routine clinical and laboratory follow-up was performed at baseline, week 4, 12, and every 12 weeks thereafter. Data were censored at week 96.
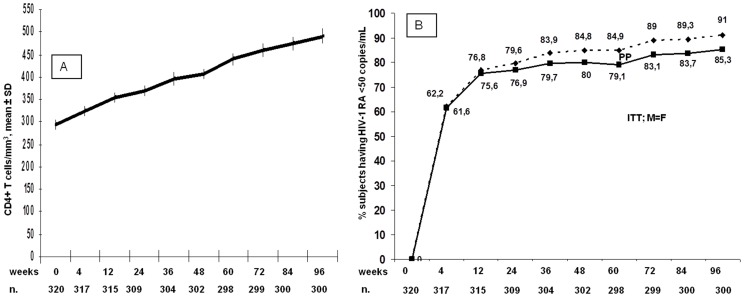
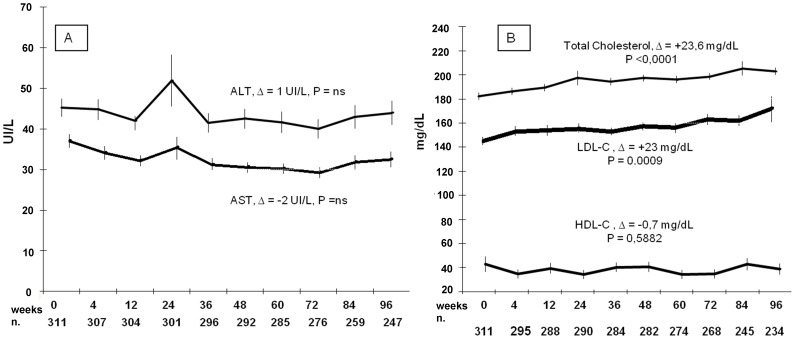
Out of 320 patients enrolled, 292 (91.25%) subjects maintained their initial regimen for 96 weeks; 28 discontinued prematurely for various reasons: death (11), viral failure (8), adverse events (5), loss to follow-up (3), consent withdrawal (1). Eight among these 28 subjects maintained RAL but changed the accompanying drugs. The mean CD4+ T-cell increase at week 96 was 227/mm(3); 273 out of 300 patients (91%), who were still receiving RAL at week 96, achieved viral suppression (HIV-1 RNA <50 copies/mL). When analyzing the immuno-virologic outcome according to the number of drugs used in the regimen, 2 (n = 45), 3 (n = 111), 4 (n = 124), or >4 (n = 40), CD4+ T-cell gain was similar across strata: +270, +214, +216, and +240 cells/mm(3), respectively, as was the proportion of subjects with undetectable viral load. Laboratory abnormalities (elevation of liver enzymes, total cholesterol and triglycerides) were rare, ranging from 0.9 to 3.1%. The mean 96-week total cholesterol increase was 23.6 mg/dL.
In a routine clinical setting, a RAL-based regimen allowed most patients in salvage therapy to achieve optimal viral suppression for at least 96 weeks, with relevant immunologic gain and very few adverse events.
在注册试验中已证明拉替拉韦(RAL)-包括方案在高度预处理的 HIV-1 感染患者中的长期疗效。然而,很少有研究在常规临床环境中评估其持久性。
入组接受 RAL 为基础的挽救治疗方案的有抗逆转录病毒治疗经验的患者。在基线、第 4、12 周和此后每 12 周进行常规临床和实验室随访。数据截止至第 96 周。
在入组的 320 例患者中,292 例(91.25%)患者维持初始方案 96 周;28 例因各种原因提前终止治疗:死亡(11 例)、病毒失败(8 例)、不良事件(5 例)、失访(3 例)、退出(1 例)。这 28 例中有 8 例继续使用 RAL,但更换了伴随药物。第 96 周时平均 CD4+T 细胞增加 227/mm3;在第 96 周仍接受 RAL 的 300 例患者中,273 例(91%)患者达到病毒抑制(HIV-1 RNA<50 拷贝/ml)。当根据方案中使用的药物数量分析免疫病毒学结果时,2(n = 45)、3(n = 111)、4(n = 124)或>4(n = 40)种药物,CD4+T 细胞增加相似:分别为+270、+214、+216 和+240 个细胞/mm3,病毒载量不可检测的患者比例也相似。实验室异常(肝酶升高、总胆固醇和甘油三酯升高)罕见,范围为 0.9 至 3.1%。96 周时平均总胆固醇增加 23.6mg/dL。
在常规临床环境中,RAL 为基础的方案使大多数接受挽救治疗的患者至少在 96 周内达到最佳病毒抑制,具有显著的免疫获益和很少的不良事件。