Department of Internal Medicine, Yonsei University College of Medicine, Seoul, South Korea.
Cardiovasc Diabetol. 2012 Jul 18;11:83. doi: 10.1186/1475-2840-11-83.
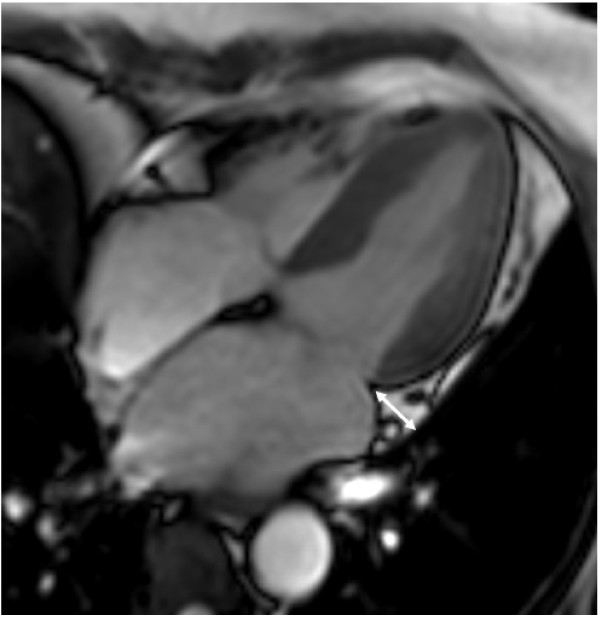
We used cardiovascular magnetic resonance (CMR) to investigate the association between epicardial adipose tissue (EAT) thickness and silent myocardial ischemia, as well as coronary artery stenosis, in asymptomatic type 2 diabetic patients.
The study included 100 type 2 diabetic subjects (51 male and 49 female; mean age: 56 ± 7 years). Silent myocardial ischemia, as determined by CMR, was defined as evidence of inducible ischemia or myocardial infarction. Signal reduction or stenosis of ≥ 50% in the vessel diameter was used as the criteria for significant coronary artery stenosis on coronary magnetic resonance (MR) angiography.
EAT thickness was positively correlated with body mass index (BMI), waist-to-hip ratio, systolic blood pressure, postprandial glucose, fasting/postprandial triglyceride (TG), serum glycated hemoglobin (HbA1c) level, and homeostasis model assessment of insulin resistance (HOMA-IR) score. Significant coronary artery stenosis was found in 24 patients, while 14 patients had silent myocardial ischemia in CMR (1 with silent myocardial infarction, 11 with inducible ischemia, and 2 with both). EAT thickness was greater in patients who had coronary artery stenosis (13.0 ± 2.6 mm vs. 11.5 ± 2.1 mm, p = 0.01), but did not differ between the subjects with or without silent myocardial ischemia on CMR images (12.8 ± 2.1 vs. 11.7 ± 2.3 mm, p = 0.11). Multivariate logistic regression analysis indicated that EAT thickness was an independent indicator for significant coronary artery stenosis after adjusting for traditional risk factors (OR 1.403, p = 0.026).
Increased EAT thickness assessed by CMR is an independent risk factor for significant coronary artery stenosis in asymptomatic type 2 diabetes. However, EAT thickness was not associated with silent myocardial ischemia.
我们使用心血管磁共振(CMR)研究了心外膜脂肪组织(EAT)厚度与无症状 2 型糖尿病患者的无症状性心肌缺血和冠状动脉狭窄之间的关系。
该研究纳入了 100 例 2 型糖尿病患者(男 51 例,女 49 例;平均年龄:56±7 岁)。CMR 确定的无症状性心肌缺血定义为可诱导缺血或心肌梗死的证据。冠状动脉磁共振血管造影(CMR-Angiography)上≥50%的血管直径信号减少或狭窄被用作冠状动脉狭窄的标准。
EAT 厚度与体重指数(BMI)、腰臀比、收缩压、餐后血糖、空腹/餐后甘油三酯(TG)、糖化血红蛋白(HbA1c)水平和胰岛素抵抗稳态模型评估(HOMA-IR)评分呈正相关。24 例患者存在明显的冠状动脉狭窄,14 例患者在 CMR 上有无症状性心肌缺血(1 例无症状性心肌梗死,11 例可诱导性缺血,2 例同时存在)。有冠状动脉狭窄的患者 EAT 厚度更大(13.0±2.6mm 比 11.5±2.1mm,p=0.01),但在 CMR 图像上有无无症状性心肌缺血的患者之间无差异(12.8±2.1mm 比 11.7±2.3mm,p=0.11)。多变量 logistic 回归分析表明,在校正传统危险因素后,EAT 厚度是冠状动脉显著狭窄的独立指标(OR 1.403,p=0.026)。
CMR 评估的 EAT 厚度增加是无症状 2 型糖尿病患者冠状动脉显著狭窄的独立危险因素。然而,EAT 厚度与无症状性心肌缺血无关。