Critical Care Division, Department of Anesthesia, Perioperative and Pain Medicine, Children's Hospital Boston, and Department of Anesthesia, Harvard Medical School, Boston, MA 02115, USA.
Crit Care Med. 2012 Oct;40(10):2883-9. doi: 10.1097/CCM.0b013e31825bc54d.
In the Fluid and Catheter Treatment Trial (NCT00281268), adults with acute lung injury randomized to a conservative vs. liberal fluid management protocol had increased days alive and free of mechanical ventilator support (ventilator-free days). Recruiting sufficient children with acute lung injury into a pediatric trial is challenging. A Bayesian statistical approach relies on the adult trial for the a priori effect estimate, requiring fewer patients. Preparing for a Bayesian pediatric trial mirroring the Fluid and Catheter Treatment Trial, we aimed to: 1) identify an inverse association between fluid balance and ventilator-free days; and 2) determine if fluid balance over time is more similar to adults in the Fluid and Catheter Treatment Trial liberal or conservative arms.
Multicentered retrospective cohort study.
Five pediatric intensive care units.
Mechanically ventilated children (age≥1 month to <18 yrs) with acute lung injury admitted in 2007-2010.
None.
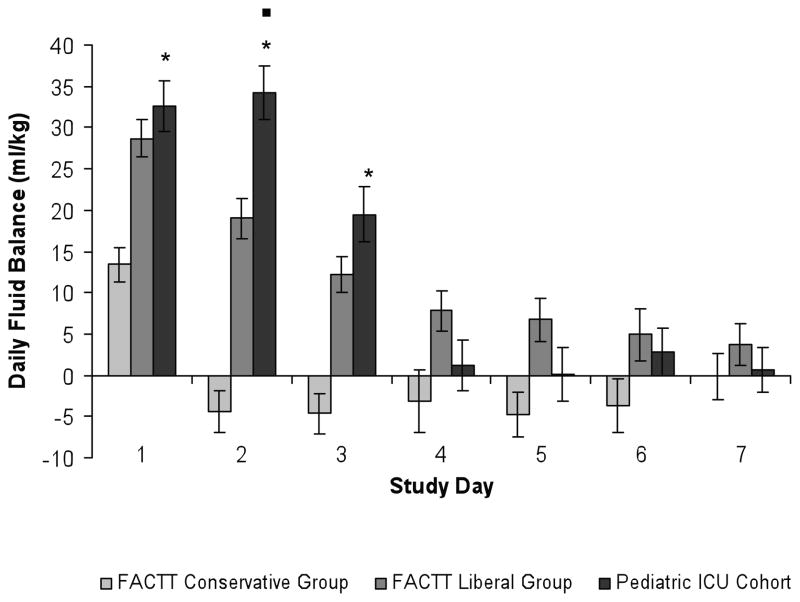
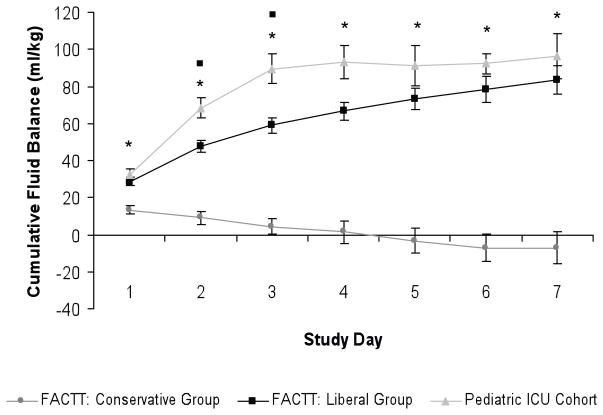
Fluid intake, output, and net fluid balance were collected on days 1-7 in 168 children with acute lung injury (median age 3 yrs, median PaO2/FIO2 138) and weight-adjusted (mL/kg). Using multivariable linear regression to adjust for age, gender, race, admission day illness severity, PaO2/FIO2, and vasopressor use, increasing cumulative fluid balance (mL/kg) on day 3 was associated with fewer ventilator-free days (p=.02). Adjusted for weight, daily fluid balance on days 1-3 and cumulative fluid balance on days 1-7 were higher in these children compared to adults in the Fluid and Catheter Treatment Trial conservative arm (p<.001, each day) and was similar to adults in the liberal arm.
Increasing fluid balance on day 3 in children with acute lung injury at these centers is independently associated with fewer ventilator-free days. Our findings and the similarity of fluid balance patterns in our cohort to adults in the Fluid and Catheter Treatment Trial liberal arm demonstrate the need to determine whether a conservative fluid management strategy improves clinical outcomes in children with acute lung injury and support a Bayesian trial mirroring the Fluid and Catheter Treatment Trial.
在液体和导管治疗试验(NCT00281268)中,随机分配到保守液体管理方案与宽松液体管理方案的急性肺损伤成人患者的存活天数和无机械通气支持天数(无呼吸机天数)增加。招募足够数量的急性肺损伤儿童参与儿科试验具有挑战性。贝叶斯统计方法依赖于成人试验的先验效应估计,因此需要的患者较少。为了筹备与液体和导管治疗试验相似的贝叶斯儿科试验,我们旨在:1)确定液体平衡与无呼吸机天数之间存在反比关系;2)确定随着时间的推移,液体平衡是否与液体和导管治疗试验中的宽松或保守治疗组更相似。
多中心回顾性队列研究。
五个儿科重症监护病房。
2007 年至 2010 年入住的患有急性肺损伤的机械通气儿童(年龄≥1 个月至<18 岁)。
无。
共纳入 168 例急性肺损伤患儿(中位年龄 3 岁,中位 PaO2/FIO2 为 138),收集了第 1-7 天的液体摄入、液体输出和净液体平衡,按体重调整(mL/kg)。使用多变量线性回归校正年龄、性别、种族、入院日疾病严重程度、PaO2/FIO2 和血管加压素使用,结果发现第 3 天累积液体平衡(mL/kg)增加与无呼吸机天数减少相关(p=.02)。校正体重后,这些患儿的第 1-3 天的每日液体平衡和第 1-7 天的累积液体平衡均高于液体和导管治疗试验保守组的成人(p<.001,每天),与宽松组的成人相似。
在这些中心,急性肺损伤患儿第 3 天的液体平衡增加与无呼吸机天数减少独立相关。我们的发现以及我们队列的液体平衡模式与液体和导管治疗试验宽松组成人相似,这表明需要确定在急性肺损伤患儿中采用保守的液体管理策略是否能改善临床结局,并支持开展与液体和导管治疗试验相类似的贝叶斯试验。