Department of Hematology, Nanfang Hospital, Southern Medical University, Guangzhou 510515, China.
J Hematol Oncol. 2012 Aug 2;5:46. doi: 10.1186/1756-8722-5-46.
Intensified conditioning regimens (increasing the intensity of standard myeloablative conditioning) for hematological malignancies in allogeneic hematopoietic stem cell transplantation (allo-HSCT) could reduce the relapse rate of the underlying disease, but it might simultaneously increase the transplant-related mortality including the mortality of infections. To explore whether intensified conditioning affected Epstein-Barr virus (EBV) and cytomegalovirus (CMV) infections, 185 patients undergoing allo-HSCT were enrolled.
A total of 104 cases received standard and 81 intensified conditioning. Cyclosporine A (CsA) withdrawal and/or donor lymphocyte infusion (DLI) were conducted in high-risk patients. The EBV-DNA and CMV-DNA levels of blood were monitored regularly by quantitative real-time polymerase chain reaction (RQ-PCR) and immune reconstitution of recipients were analyzed by flow cytometry.
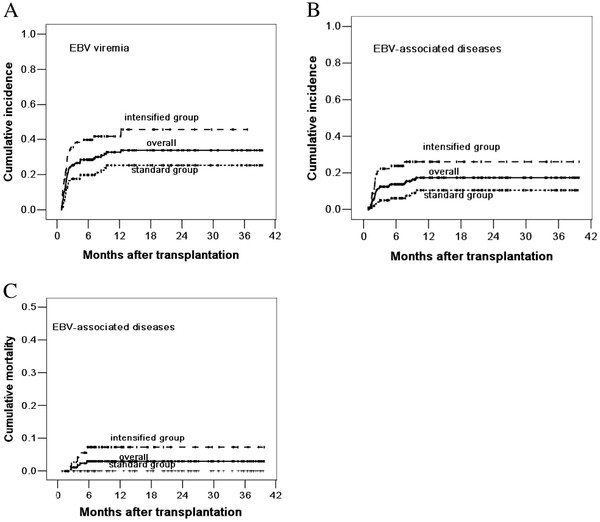
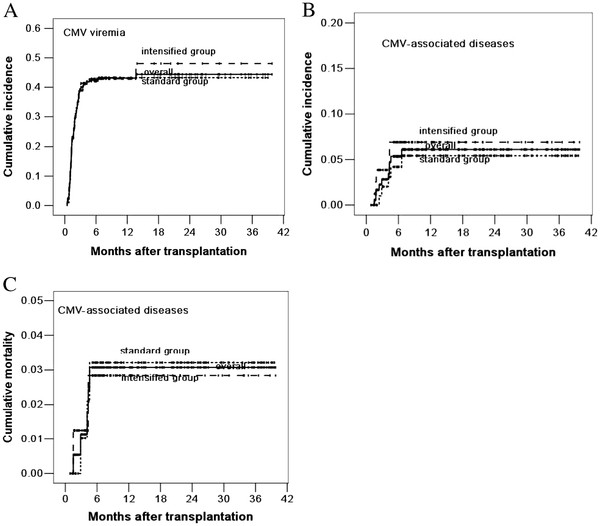
The 3-year cumulative incidence of EBV viremia, EBV-associated diseases and mortality of EBV-associated diseases were 25.3% ± 4.6%, 10.5% ± 3.4% and 0.0% ± 0.0% in the standard group, compared with 45.6% ± 6.5%, 26.0% ±5.3% and 7.3% ± 3.1% in the intensified group (P = 0.002, P = 0.002, P = 0.008). The 3-year cumulative incidence of CMV viremia and CMV-associated diseases, mortality of CMV-associated diseases and incidence of bacterial and fungal infections were similar between the two groups (P = 0.855, P = 0.581, P = 0.933, P = 0.142, P = 0.182, respectively). Multivariate analysis showed that intensified conditioning was one of the risk factors for EBV viremia and EBV-associated diseases (P = 0.037, P = 0.037), but it had no effects on CMV infections. The percentage of CD4+ T cells and CD4+/CD8+ ratio at 3 months post-transplantation were lower in the intensified group (P = 0.032, P = 0.022). The 3-year OS and DFS in the standard group were 62.2% ± 5.8% and 60.6% ± 5.6%, compared with 51.6% ± 6.2% and 51.1% ± 5.9% in the intensified group (P = 0.029, P = 0.063).
Intensified conditioning represents a promising approach for high-risk hematological malignancies, although it affects early immune reconstitution of recipients and increases the incidence and mortality of EBV infections.
异基因造血干细胞移植(allo-HSCT)中强化预处理方案(增加标准骨髓清除性预处理的强度)可降低基础疾病的复发率,但可能同时增加移植相关死亡率,包括感染相关死亡率。为了探讨强化预处理是否会影响 EBV 和 CMV 感染,本研究纳入了 185 例接受 allo-HSCT 的患者。
共 104 例患者接受标准预处理,81 例患者接受强化预处理。高危患者接受环孢素 A(CsA)停药和/或供者淋巴细胞输注(DLI)。通过实时定量聚合酶链反应(RQ-PCR)定期监测血液 EBV-DNA 和 CMV-DNA 水平,并通过流式细胞术分析受者的免疫重建情况。
标准组和强化组的 EBV 血症、 EBV 相关疾病和 EBV 相关疾病死亡率的 3 年累积发生率分别为 25.3%±4.6%、10.5%±3.4%和 0.0%±0.0%,45.6%±6.5%、26.0%±5.3%和 7.3%±3.1%(P=0.002,P=0.002,P=0.008)。两组患者的 CMV 血症、CMV 相关疾病、CMV 相关疾病死亡率以及细菌和真菌感染发生率相似(P=0.855,P=0.581,P=0.933,P=0.142,P=0.182)。多因素分析显示,强化预处理是 EBV 血症和 EBV 相关疾病的危险因素之一(P=0.037,P=0.037),但对 CMV 感染无影响。移植后 3 个月,强化组 CD4+T 细胞百分比和 CD4+/CD8+比值较低(P=0.032,P=0.022)。标准组的 3 年 OS 和 DFS 分别为 62.2%±5.8%和 60.6%±5.6%,强化组分别为 51.6%±6.2%和 51.1%±5.9%(P=0.029,P=0.063)。
强化预处理是高危血液系统恶性肿瘤的一种有前途的方法,尽管它会影响受者的早期免疫重建,并增加 EBV 感染的发生率和死亡率。