Division of Cardiology, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Gangnam-gu, Seoul 135-710, Korea.
Yonsei Med J. 2012 Sep;53(5):906-14. doi: 10.3349/ymj.2012.53.5.906.
The optimum loading dose of clopidogrel has not been established in Asian patients with ST-segment elevation myocardial infarction (STEMI) undergoing primary percutaneous coronary intervention (PCI). Our aim was to evaluate the impact of different clopidogrel loading doses on short- and long-term clinical outcomes in Asian STEMI patients undergoing primary PCI.
We studied 691 STEMI patients undergoing primary PCI, loaded with 600 mg (n=381) or 300 mg (n=310) of clopidogrel. The primary outcome was major adverse cardiac events (MACEs), defined as a composite of all-cause death, reinfarction, or target vessel revascularization (TVR).
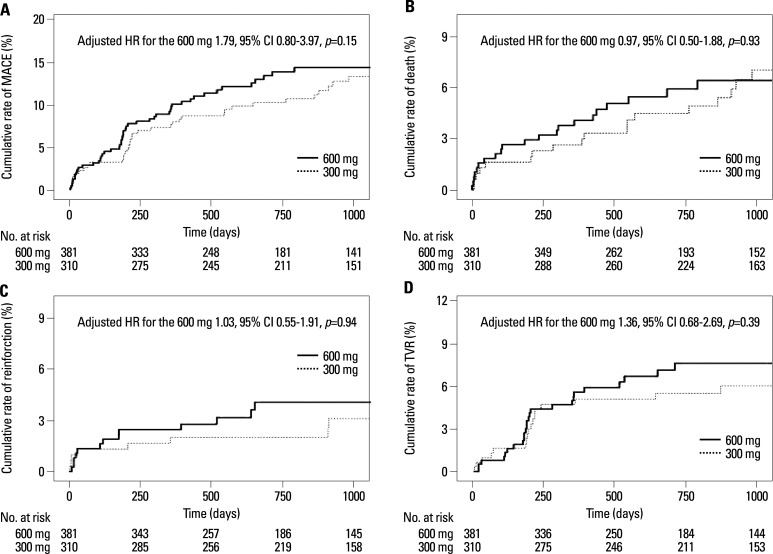
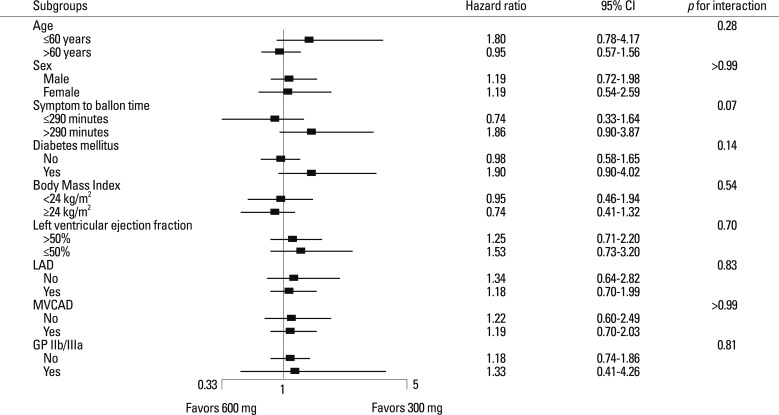
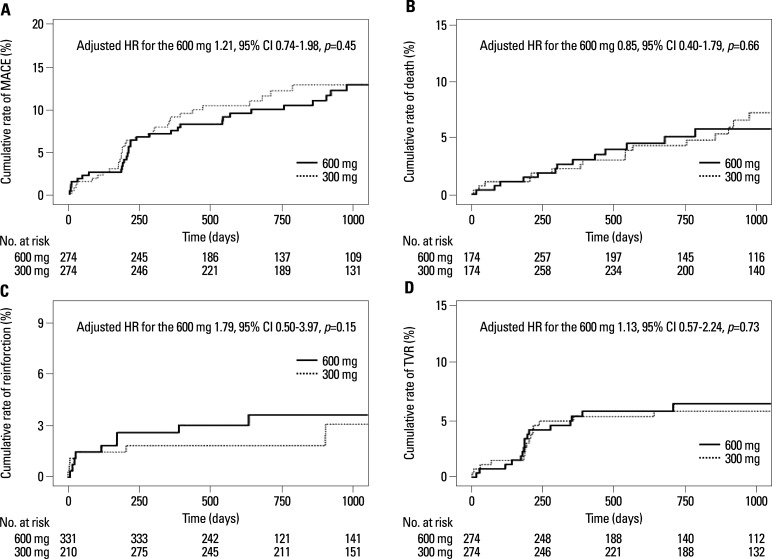
Baseline clinical and peri-procedural characteristics were mostly comparable between the 600 mg and 300 mg groups. There were no differences in 1 month MACEs as well as all-cause death, reinfarction, TVR, and stent thrombosis between the two groups. After a median follow-up of 921 days, MACEs [adjusted hazard ratio (HR) for the 600 mg group 1.79, 95% confidence interval (CI): 0.80-3.97, p=0.153], all-cause death (adjusted HR for the 600 mg group 0.97, 95% CI: 0.50-1.88, p=0.928), reinfarction (adjusted HR for the 600 mg group 1.03, 95% CI: 0.55-1.91, p=0.937), and TVR (adjusted HR for the 600 mg group 1.36, 95% CI: 0.68-2.69, p=0.388) did not differ between the two groups. These results were reliable even after analysis of propensity score-matched population, and were also constant among various subgroups.
A 600 mg loading dose of clopidogrel did not result in better short- and long-term clinical outcomes in Asian STEMI patients undergoing primary PCI.
在接受直接经皮冠状动脉介入治疗(PCI)的亚洲 ST 段抬高型心肌梗死(STEMI)患者中,氯吡格雷的最佳负荷剂量尚未确定。我们的目的是评估亚洲 STEMI 患者接受直接 PCI 时不同氯吡格雷负荷剂量对短期和长期临床结局的影响。
我们研究了 691 例接受直接 PCI 的 STEMI 患者,分别给予 600mg(n=381)或 300mg(n=310)氯吡格雷负荷量。主要不良心脏事件(MACE)为主要终点,定义为全因死亡、再梗死或靶血管血运重建(TVR)的复合终点。
两组患者的基线临床和围术期特征基本相似。两组 1 个月时的 MACE 发生率、全因死亡、再梗死、TVR 和支架血栓形成无差异。中位随访 921 天后,MACE[600mg 组调整后的危险比(HR)为 1.79,95%置信区间(CI):0.80-3.97,p=0.153]、全因死亡(600mg 组调整后的 HR 为 0.97,95%CI:0.50-1.88,p=0.928)、再梗死(600mg 组调整后的 HR 为 1.03,95%CI:0.55-1.91,p=0.937)和 TVR(600mg 组调整后的 HR 为 1.36,95%CI:0.68-2.69,p=0.388)差异无统计学意义。即使在倾向评分匹配人群的分析中,这些结果也是可靠的,而且在各种亚组中也是一致的。
在亚洲 STEMI 患者接受直接 PCI 时,600mg 氯吡格雷负荷剂量并未带来更好的短期和长期临床结局。