Center of Gastroenterology, Hospital Cuf Infante Santo, Travessa do Castro n º 3, 1350-070, Lisbon, Portugal.
BMC Gastroenterol. 2012 Aug 9;12:103. doi: 10.1186/1471-230X-12-103.
Endoscopic biliary drainage of hilar cholangiocarcinoma is controversial with respect to the optimal types of stents and the extent of drainage. This study evaluated endoscopic palliation in patients with hilar cholangiocarcinoma using self-expandable metallic stents (SEMS) and plastic stents (PS).We also compared unilateral and bilateral stent placement according to the Bismuth classification.
Data on 480 patients receiving endoscopic biliary drainage for hilar cholangiocarcinoma between September 1995 and December 2010 were retrospectively reviewed to evaluate the following outcome parameters: technical success (TS), functional success (FS), early and late complications, stent patency and survival. Patients were followed from stent insertion until death or stent occlusion. Patients were divided into 3 groups according to the Bismuth classification (Group 1, type I; Group 2, type II; Group 3, type ≥ III).
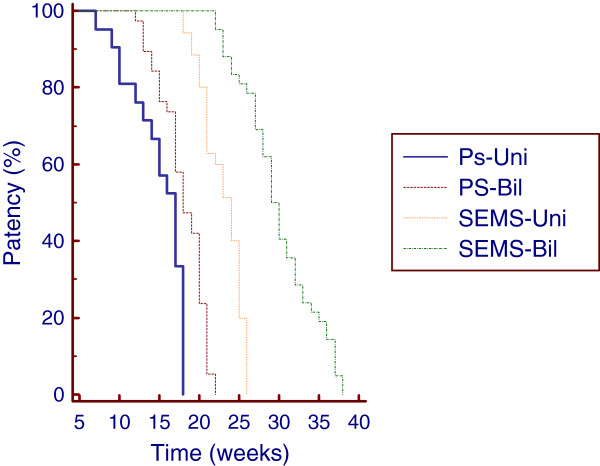
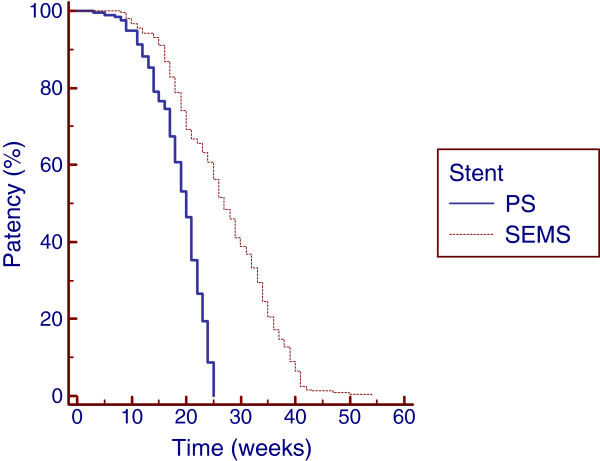
The initial stent insertion was successful in 450 (93.8%) patients. TS was achieved in 204 (88.3%) patients treated with PS and in 246 (98.8%) patients palliated with SEMS (p < 0.001). In the intention-to-treat (ITT) analysis, the FS in patients treated with SEMS (97.9%) was significantly higher than in patients treated with PS (84.8%) (p < 0.001). Late complications occurred in 115 (56.4%) patients treated with PS and 60 (24.4%) patients treated with SEMS (p < 0.001). The median duration of stent patency in weeks (w) were as follows: 20 w in patients palliated with PS and 27 w in patients treated with SEMS (p < 0.0001). In Group 2, the median duration of PS patency was 17 w and 18 w for unilateral and bilateral placement, respectively (p = 0.0004); the median duration of SEMS patency was 24 w and 29 w for unilateral and bilateral placement, respectively (p < 0.0001). Multivariate analysis using the Poisson regression showed that SEMS placement (B = 0.48; P < 0.01) and bilateral deployment (B = 0.24; P < 0.01) were the only independent prognostic factors associated with stent patency.
SEMS insertion for the palliation of hilar cholangiocarcinoma offers higher technical and clinical success rates in the ITT analysis as well as lower complication rates and a superior cumulative stent patency when compared with PS placement in all Bismuth classifications. The cumulative patency of bilateral SEMS or PS stents was significantly higher than that of unilateral SEMS or PS stents, with lower occlusion rates in Bismuth II patients.
对于肝门部胆管癌的内镜下胆道引流,支架的最佳类型和引流的范围存在争议。本研究使用自膨式金属支架(SEMS)和塑料支架(PS)评估了肝门部胆管癌患者的内镜姑息治疗。我们还根据 Bismuth 分类比较了单侧和双侧支架放置。
回顾性分析 1995 年 9 月至 2010 年 12 月期间接受内镜胆道引流治疗的 480 例肝门部胆管癌患者的数据,以评估以下结局参数:技术成功率(TS)、功能成功率(FS)、早期和晚期并发症、支架通畅率和生存率。从支架置入开始随访患者,直至死亡或支架闭塞。患者根据 Bismuth 分类(1 型,Group 1;2 型,Group 2;≥3 型,Group 3)分为 3 组。
450 例(93.8%)患者初始支架置入成功。PS 治疗的 204 例(88.3%)和 SEMS 治疗的 246 例(98.8%)患者的 TS 均达到(p < 0.001)。意向治疗(ITT)分析中,SEMS 治疗的 FS(97.9%)显著高于 PS 治疗(84.8%)(p < 0.001)。PS 治疗的 115 例(56.4%)和 SEMS 治疗的 60 例(24.4%)患者发生晚期并发症(p < 0.001)。PS 治疗的中位支架通畅时间为 20 周,SEMS 治疗的中位支架通畅时间为 27 周(p < 0.0001)。在 Group 2 中,PS 通畅时间的中位值分别为 17 周和单侧、双侧放置的 18 周(p = 0.0004);SEMS 通畅时间的中位值分别为 24 周和单侧、双侧放置的 29 周(p < 0.0001)。多变量分析采用泊松回归显示,SEMS 放置(B = 0.48;P < 0.01)和双侧放置(B = 0.24;P < 0.01)是与支架通畅率相关的唯一独立预后因素。
在所有 Bismuth 分类中,与 PS 放置相比,SEMS 置入治疗肝门部胆管癌的 ITT 分析中技术和临床成功率更高,并发症发生率更低,累积支架通畅率更高。双侧 SEMS 或 PS 支架的累积通畅率明显高于单侧 SEMS 或 PS 支架,Bismuth II 型患者的支架闭塞率较低。