University of Tennessee Health Science Center, Memphis, TN 38163, USA.
Diagn Pathol. 2012 Aug 21;7:110. doi: 10.1186/1746-1596-7-110.
Determining the primary site of metastatic cancer with confidence can be challenging. Pathologists commonly use a battery of immunohistochemical (IHC) stains to determine the primary site. Gene expression profiling (GEP) has found increasing use, particularly in the most difficult cases. In this pilot study, a direct comparison between GEP and IHC-guided methods was performed.
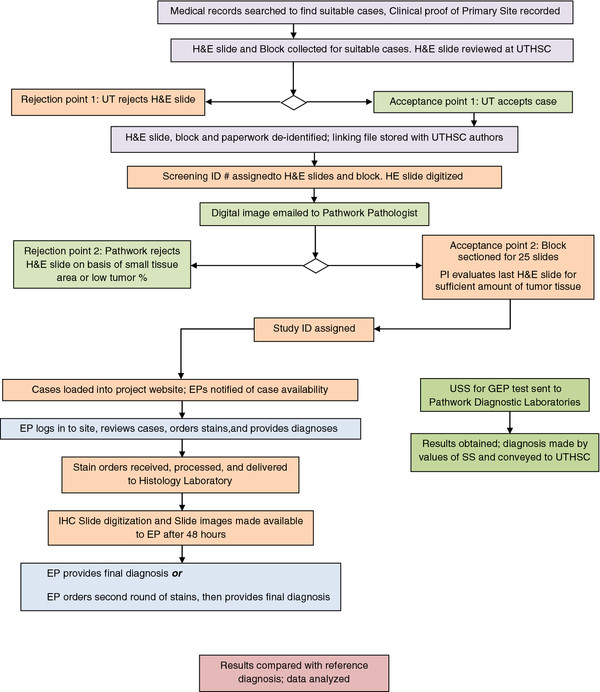
Ten archived formalin-fixed paraffin embedded metastatic tumor samples for which the primary site had been clinically determined were selected. Five pathologists who were blinded to the diagnosis were asked to determine the primary site using IHC and other stains selected from a panel of 84 stains. Each pathologist was provided patient sex, biopsy site and gross sample description only. Slides were digitized using ScanScope®XT at 0.25 μm/pixel. Each evaluating pathologist was allowed to provide a diagnosis in three stages: initial (after reviewing the H&E image), intermediate (after reviewing images from the first batch of stains) and final diagnosis (after the second batch of stains if requested). GEP was performed using the only FDA-cleared test for this intended use, the Pathwork Tissue of Origin Test. No sample information was provided for GEP testing except for patient sex. Results were reported as the tumor tissue type with the highest similarity score.
In this feasibility study, GEP determined the correct primary site in 9 of the 10 cases (90%), compared to the IHC-guided method which determined the correct primary site for 32 of 50 case evaluations (average 64%, range 50% to 80%). The five pathologists directing the IHC-guided method ordered an average of 8.8 stains per case (range 1 to 18). GEP required an average of 3 slides per case (range 1 to 4).
Results of the pilot study suggest that GEP provides correct primary site identification in a higher percentage of metastatic cases than IHC-guided methods, and uses less tissue. A larger comparative effectiveness study using this study design is needed to confirm the results.
The virtual slide(s) for this article can be found here: http://www.diagnosticpathology.diagnomx.eu/vs/1749854104745508.
有信心确定转移性癌症的原发部位可能具有挑战性。病理学家通常使用一系列免疫组织化学(IHC)染色来确定原发部位。基因表达谱(GEP)的使用越来越多,特别是在最困难的情况下。在这项初步研究中,对 GEP 与 IHC 引导方法进行了直接比较。
选择了 10 个存档的福尔马林固定石蜡包埋的转移性肿瘤样本,这些样本的原发部位已通过临床确定。5 位对诊断结果不知情的病理学家被要求使用 IHC 以及从 84 种染色剂中选择的其他染色剂来确定原发部位。每位病理学家仅提供患者性别、活检部位和大体样本描述。使用 ScanScope®XT 以 0.25 μm/pixel 的分辨率对切片进行数字化。每位评估病理学家都可以分三个阶段提供诊断:初始诊断(在查看 H&E 图像后)、中间诊断(在查看第一批染色剂的图像后)和最终诊断(如果需要,在第二批染色剂后)。GEP 使用唯一获得 FDA 批准用于此预期用途的测试,即 Pathwork 组织起源测试。除了患者性别外,没有提供 GEP 测试的任何样本信息。结果以最高相似度评分的肿瘤组织类型报告。
在这项可行性研究中,GEP 在 10 例中的 9 例(90%)中确定了正确的原发部位,而 IHC 引导方法在 50 例评估中的 32 例(平均 64%,范围 50%至 80%)中确定了正确的原发部位。指导 IHC 引导方法的 5 位病理学家平均为每个病例订购了 8.8 种染色剂(范围为 1 至 18)。GEP 平均每个病例需要 3 张切片(范围为 1 至 4)。
初步研究结果表明,与 IHC 引导方法相比,GEP 在更高比例的转移性病例中提供了正确的原发部位识别,并且使用的组织更少。需要使用这种研究设计进行更大的比较有效性研究来确认结果。
本文的虚拟幻灯片可以在此处找到:http://www.diagnosticpathology.diagnomx.eu/vs/1749854104745508。