Department of Immunology; The Netherlands Cancer Institute; Amsterdam, The Netherlands.
Oncoimmunology. 2012 Aug 1;1(5):609-617. doi: 10.4161/onci.20226.
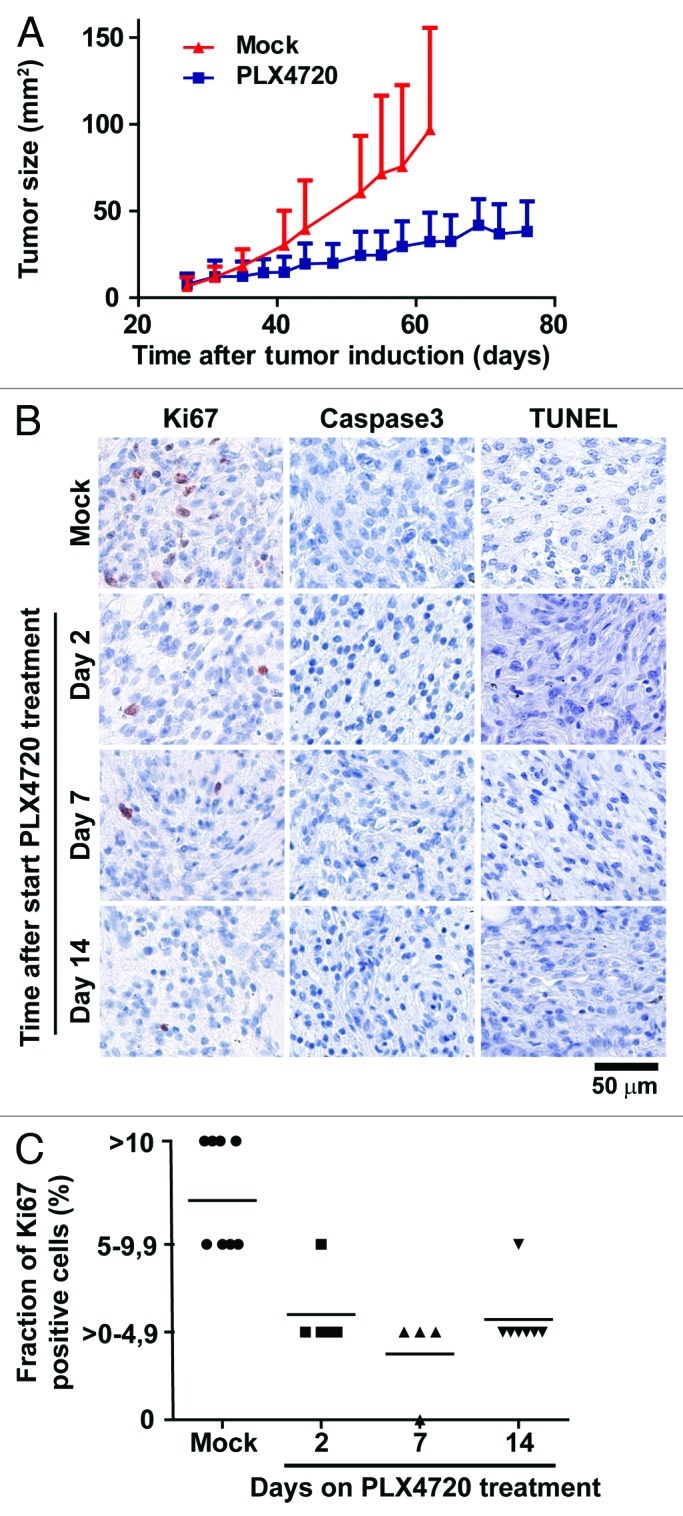
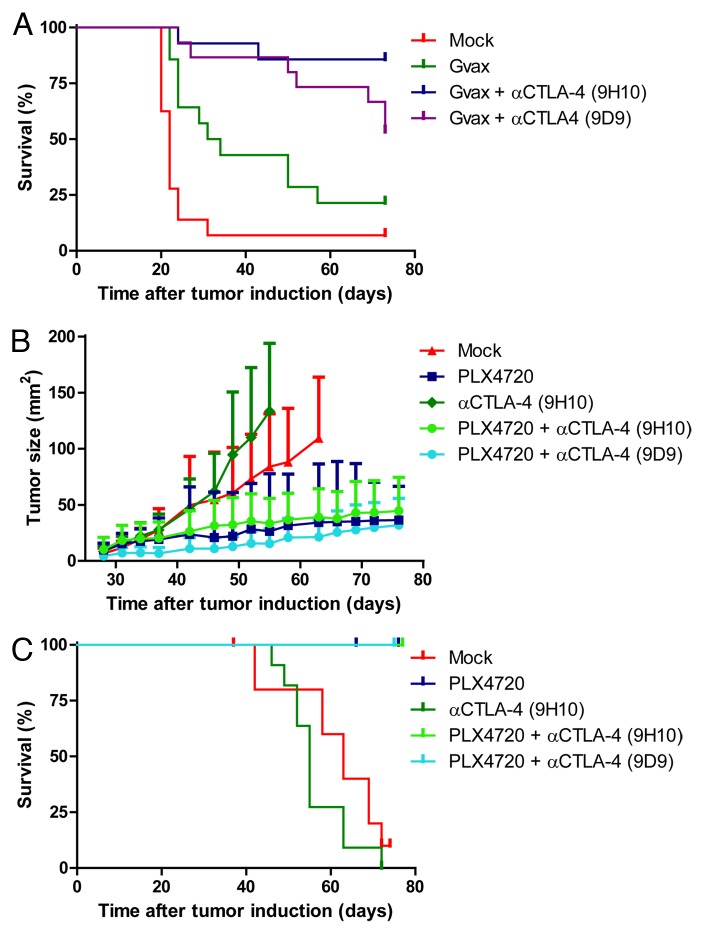
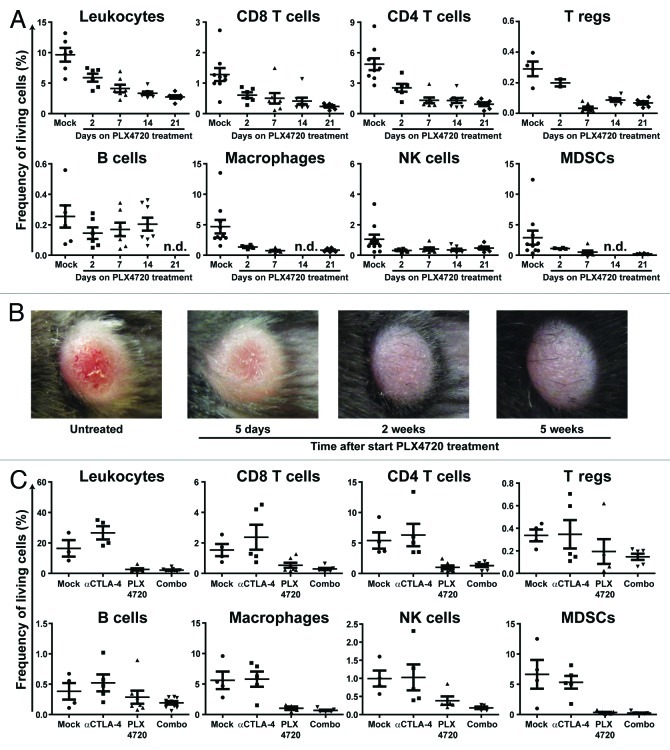
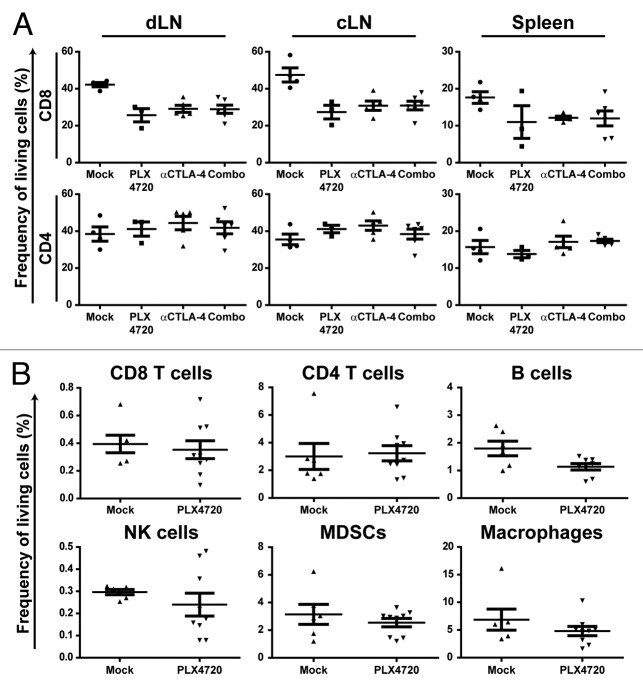
The development of targeted therapies and immunotherapies has markedly advanced the treatment of metastasized melanoma. While treatment with selective BRAF(V600E) inhibitors (like vemurafenib or dabrafenib) leads to high response rates but short response duration, CTLA-4 blocking therapies induce sustained responses, but only in a limited number of patients. The combination of these diametric treatment approaches may further improve survival, but pre-clinical data concerning this approach is limited. We investigated, using Tyr::CreER(T2)PTEN(F-/-)BRAF(F-V600E/+) inducible melanoma mice, whether BRAF(V600E) inhibition can synergize with anti-CTLA-4 mAb treatment, focusing on the interaction between the BRAF(V600E) inhibitor PLX4720 and the immune system. While PLX4720 treatment strongly decreased tumor growth, it did not induce cell death in BRAF(V600E)/PTEN(-/-) melanomas. More strikingly, PLX4720 treatment led to a decreased frequency of tumor-resident T cells, NK-cells, MDSCs and macrophages, which could not be restored by the addition of anti-CTLA-4 mAb. As this effect was not observed upon treatment of BRAF wild-type B16F10 tumors, we conclude that the decreased frequency of immune cells correlates to BRAF(V600E) inhibition in tumor cells and is not due to an off-target effect of PLX4720 on immune cells. Furthermore, anti-CTLA-4 mAb treatment of inducible melanoma mice treated with PLX4720 did not result in enhanced tumor control, while anti-CTLA-4 mAb treatment did improve the effect of tumor-vaccination in B16F10-inoculated mice. Our data suggest that vemurafenib may negatively affect the immune activity within the tumor. Therefore, the potential effect of targeted therapy on the tumor-microenvironment should be taken into consideration in the design of clinical trials combining targeted and immunotherapy.
靶向治疗和免疫疗法的发展显著改善了转移性黑色素瘤的治疗效果。选择性 BRAF(V600E)抑制剂(如vemurafenib 或 dabrafenib)的治疗可导致高反应率,但反应持续时间短,CTLA-4 阻断疗法可诱导持续反应,但仅在少数患者中。这些截然相反的治疗方法的联合可能进一步提高生存率,但关于这种方法的临床前数据有限。我们使用 Tyr::CreER(T2)PTEN(F-/-)BRAF(F-V600E/+)诱导性黑色素瘤小鼠进行了研究,以确定 BRAF(V600E)抑制是否可以与抗 CTLA-4 mAb 治疗协同作用,重点关注 BRAF(V600E)抑制剂 PLX4720 与免疫系统之间的相互作用。虽然 PLX4720 治疗强烈抑制肿瘤生长,但不会诱导 BRAF(V600E)/PTEN(-/-)黑色素瘤细胞死亡。更引人注目的是,PLX4720 治疗导致肿瘤内驻留的 T 细胞、NK 细胞、MDSC 和巨噬细胞的频率降低,而添加抗 CTLA-4 mAb 则不能恢复这种频率。由于这种作用在 BRAF 野生型 B16F10 肿瘤的治疗中没有观察到,我们得出结论,免疫细胞频率的降低与肿瘤细胞中的 BRAF(V600E)抑制有关,而不是 PLX4720 对免疫细胞的脱靶作用所致。此外,PLX4720 治疗的诱导性黑色素瘤小鼠的抗 CTLA-4 mAb 治疗并未导致肿瘤控制增强,而抗 CTLA-4 mAb 治疗可改善 B16F10 接种小鼠的肿瘤疫苗接种效果。我们的数据表明,vemurafenib 可能会对肿瘤内的免疫活性产生负面影响。因此,在设计联合靶向和免疫治疗的临床试验时,应考虑靶向治疗对肿瘤微环境的潜在影响。