Group Health Research Institute, 1730 Minor Ave, Ste 1600, Seattle, WA 98101, USA.
J Natl Cancer Inst. 2012 Sep 5;104(17):1293-305. doi: 10.1093/jnci/djs317.
Clinical trials demonstrated that women treated for breast cancer with anthracycline or trastuzumab are at increased risk for heart failure and/or cardiomyopathy (HF/CM), but the generalizability of these findings is unknown. We estimated real-world adjuvant anthracycline and trastuzumab use and their associations with incident HF/CM.
We conducted a population-based, retrospective cohort study of 12,500 women diagnosed with incident, invasive breast cancer from January 1, 1999 through December 31, 2007, at eight integrated Cancer Research Network health systems. Using administrative procedure and pharmacy codes, we identified anthracycline, trastuzumab, and other chemotherapy use. We identified incident HF/CM following chemotherapy initiation and assessed risk of HF/CM with time-varying chemotherapy exposures vs no chemotherapy. Multivariable Cox proportional hazards regression models were used to estimate hazard ratios (HRs) and 95% confidence intervals (CIs) with adjustment for age at diagnosis, stage, Cancer Research Network site, year of diagnosis, radiation therapy, and comorbidities.
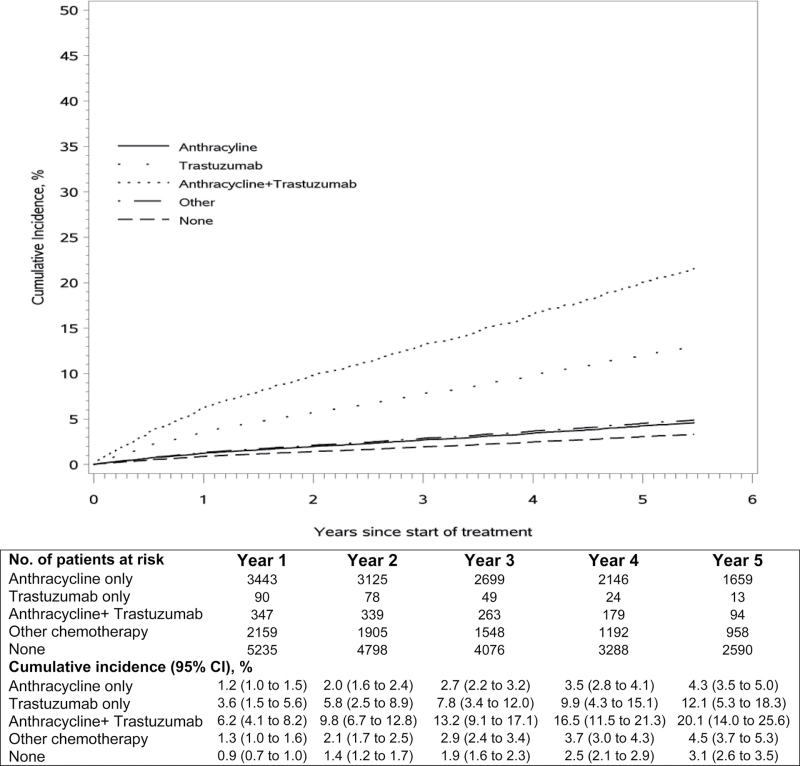
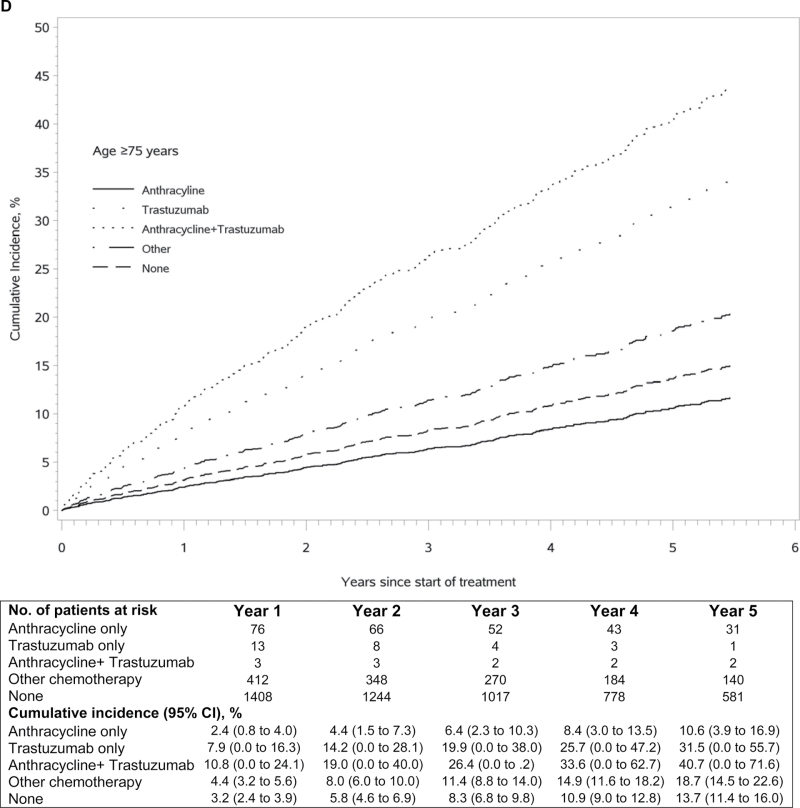
Among 12 500 women (mean age = 60 years, range = 22-99 years), 29.6% received anthracycline alone, 0.9% received trastuzumab alone, 3.5% received anthracycline plus trastuzumab, 19.5% received other chemotherapy, and 46.5% received no chemotherapy. Anthracycline and trastuzumab recipients were younger, with fewer comorbidities than recipients of other chemotherapy or none. Compared with no chemotherapy, the risk of HF/CM was higher in patients treated with anthracycline alone (adjusted HR = 1.40, 95% CI = 1.11 to 1.76), although the increased risk was similar to other chemotherapy (adjusted HR = 1.49, 95% CI = 1.25 to 1.77); the risk was highly increased in patients treated with trastuzumab alone (adjusted HR = 4.12, 95% CI = 2.30 to 7.42) or anthracycline plus trastuzumab (adjusted HR = 7.19, 95% CI = 5.00 to 10.35).
Anthracycline and trastuzumab were primarily used in younger, healthier women and associated with increased HF/CM risk compared with no chemotherapy. This population-based observational study complements findings from clinical trials on cancer treatment safety.
临床试验表明,接受蒽环类药物或曲妥珠单抗治疗乳腺癌的女性发生心力衰竭和/或心肌病(HF/CM)的风险增加,但这些发现的普遍性尚不清楚。我们估计了辅助蒽环类药物和曲妥珠单抗的实际使用情况及其与新发 HF/CM 的相关性。
我们对 1999 年 1 月 1 日至 2007 年 12 月 31 日期间在 8 个综合癌症研究网络健康系统中诊断出患有浸润性乳腺癌的 12500 名女性进行了一项基于人群的回顾性队列研究。我们使用行政程序和药房代码来确定蒽环类药物、曲妥珠单抗和其他化疗药物的使用情况。我们在化疗开始后确定了新发 HF/CM,并评估了与未化疗相比,随着时间推移接受化疗暴露与 HF/CM 风险之间的关系。使用多变量 Cox 比例风险回归模型,根据诊断时的年龄、分期、癌症研究网络地点、诊断年份、放疗和合并症来调整危险比(HR)和 95%置信区间(CI)。
在 12500 名女性中(平均年龄为 60 岁,范围为 22-99 岁),29.6%接受了单独的蒽环类药物治疗,0.9%接受了单独的曲妥珠单抗治疗,3.5%接受了蒽环类药物联合曲妥珠单抗治疗,19.5%接受了其他化疗,46.5%未接受化疗。与接受其他化疗或不接受化疗的患者相比,接受蒽环类药物和曲妥珠单抗治疗的患者年龄较小,合并症较少。与未接受化疗相比,单独接受蒽环类药物治疗的患者发生 HF/CM 的风险更高(调整后的 HR=1.40,95%CI=1.11 至 1.76),尽管风险增加与其他化疗相似(调整后的 HR=1.49,95%CI=1.25 至 1.77);单独接受曲妥珠单抗治疗(调整后的 HR=4.12,95%CI=2.30 至 7.42)或接受蒽环类药物联合曲妥珠单抗治疗(调整后的 HR=7.19,95%CI=5.00 至 10.35)的患者风险显著增加。
蒽环类药物和曲妥珠单抗主要用于年轻、健康的女性,与未接受化疗相比,与 HF/CM 风险增加相关。这项基于人群的观察性研究补充了癌症治疗安全性的临床试验结果。