Institute for Clinical Evaluative Sciences, Toronto, Canada.
PLoS One. 2012;7(9):e44103. doi: 10.1371/journal.pone.0044103. Epub 2012 Sep 4.
Evidence-based priority setting is increasingly important for rationally distributing scarce health resources and for guiding future health research. We sought to quantify the contribution of a wide range of infectious diseases to the overall infectious disease burden in a high-income setting.
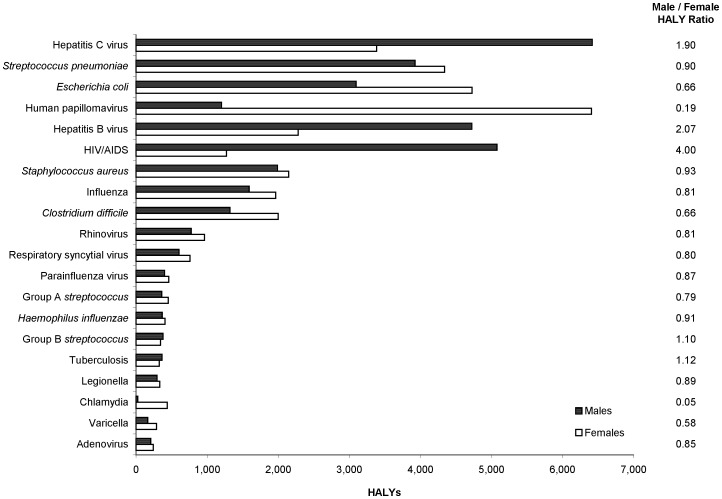
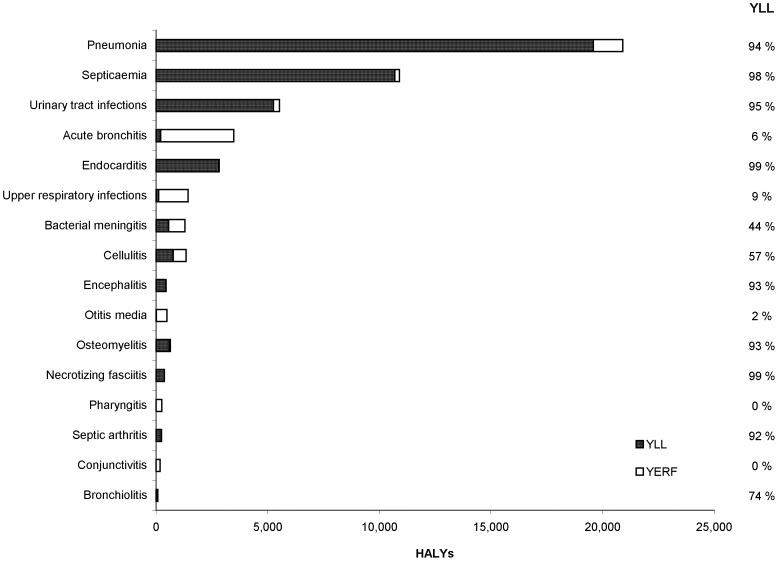
METHODOLOGY/PRINCIPAL FINDINGS: We used health-adjusted life years (HALYs), a composite measure comprising premature mortality and reduced functioning due to disease, to estimate the burden of 51 infectious diseases and associated syndromes in Ontario using 2005-2007 data. Deaths were estimated from vital statistics data and disease incidence was estimated from reportable disease, healthcare utilization, and cancer registry data, supplemented by local modeling studies and national and international epidemiologic studies. The 51 infectious agents and associated syndromes accounted for 729 lost HALYs, 44.2 deaths, and 58,987 incident cases per 100,000 population annually. The most burdensome infectious agents were: hepatitis C virus, Streptococcus pneumoniae, Escherichia coli, human papillomavirus, hepatitis B virus, human immunodeficiency virus, Staphylococcus aureus, influenza virus, Clostridium difficile, and rhinovirus. The top five, ten, and 20 pathogens accounted for 46%, 67%, and 75% of the total infectious disease burden, respectively. Marked sex-specific differences in disease burden were observed for some pathogens. The main limitations of this study were the exclusion of certain infectious diseases due to data availability issues, not considering the impact of co-infections and co-morbidity, and the inability to assess the burden of milder infections that do not result in healthcare utilization.
CONCLUSIONS/SIGNIFICANCE: Infectious diseases continue to cause a substantial health burden in high-income settings such as Ontario. Most of this burden is attributable to a relatively small number of infectious agents, for which many effective interventions have been previously identified. Therefore, these findings should be used to guide public health policy, planning, and research.
循证决策对于合理分配有限的卫生资源以及指导未来卫生研究越来越重要。我们试图量化广泛的传染病在高收入环境下对整体传染病负担的贡献。
方法/主要发现:我们使用健康调整生命年(HALYs),这是一个综合衡量指标,包含因疾病导致的过早死亡和功能下降,根据 2005-2007 年的数据,使用报告病例、医疗保健利用和癌症登记数据,以及当地建模研究和国家及国际流行病学研究来补充,对安大略省的 51 种传染病和相关综合征进行了负担评估。死亡人数是根据生命统计数据估计的,疾病发病率是根据报告病例、医疗保健利用和癌症登记数据估计的。51 种传染病病原体和相关综合征每年导致每 100,000 人口损失 729 个 HALYs、44.2 例死亡和 58,987 例新发病例。负担最重的传染病病原体是:丙型肝炎病毒、肺炎链球菌、大肠杆菌、人乳头瘤病毒、乙型肝炎病毒、人类免疫缺陷病毒、金黄色葡萄球菌、流感病毒、艰难梭菌和鼻病毒。排名前五、前十和前二十的病原体分别占传染病总负担的 46%、67%和 75%。对于某些病原体,观察到疾病负担存在明显的性别特异性差异。本研究的主要局限性是由于数据可用性问题排除了某些传染病,未考虑合并感染和合并疾病的影响,以及无法评估未导致医疗保健利用的轻度感染的负担。
结论/意义:传染病在安大略等高收入环境中继续造成重大的健康负担。这种负担主要归因于少数传染病病原体,对于这些病原体,以前已经确定了许多有效的干预措施。因此,这些发现应被用于指导公共卫生政策、规划和研究。