Institute of Cardiology, University of Bologna, Azienda Ospedaliera S, Orsola-Malpighi; Via Massarenti, 9 40138, Bologna, Italy.
BMC Cardiovasc Disord. 2012 Sep 11;12:72. doi: 10.1186/1471-2261-12-72.
A multicenter European Registry, SEARCH-MI, was instituted in the year 2002 in order to assess patients' outcomes and ICD interventions in patients with a previous MI and depressed LV function, treated with an ICD according to MADIT II results. In this analysis, we evaluate the influence of the time elapsed between last myocardial infarction (MI) and prophylactic cardioverter defibrillator (ICD) implant on device activations.
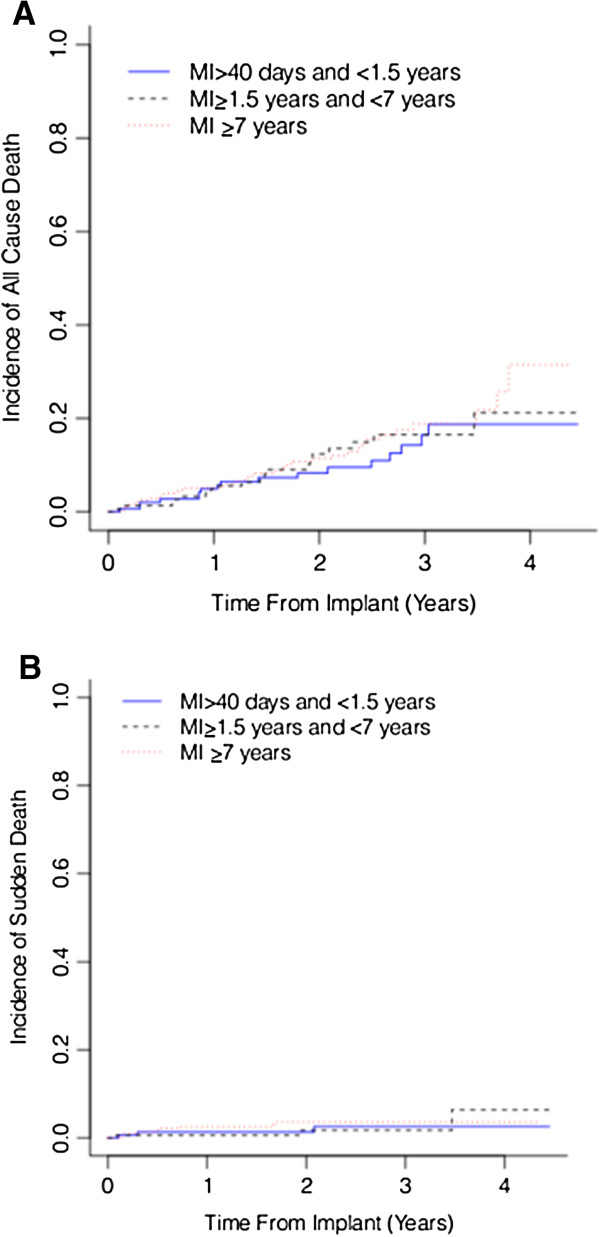
643 patients with left ventricular dysfunction (mean LVEF 26 ± 5%) and NYHA class I-III were prospectively followed for 1.8 ± 1.2 years in a multicenter registry. The population was divided into 3 groups according to the time between last MI and ICD implant: [1] from 40 days to less than 1.5 years; [2] from 1.5 to less than 7 years and [3] at least 7 years.
The cumulative incidence of ventricular tachyarrhymias and appropriate device therapy (ATP or shock) were higher in patients implanted longer time from last MI (Gray's Test p=0.002 and p=0.013 respectively). No significant differences were seen in all cause mortality (Gray's Test p=0.618) or sudden cardiac death across the MI stratification groups (Gray's Test p=0.663).
Patients implanted with an ICD longer after the MI have a higher chance of presenting ventricular tachyarrhythmias and appropriate ICD therapy, while no differences were seen in overall mortality. These observations may be important for improving patient targeting in sudden death prevention.
为了评估先前患有 MI 和左心室功能降低的患者的结局和 ICD 干预措施,并根据 MADIT II 结果用 ICD 治疗这些患者,于 2002 年建立了一个多中心欧洲注册研究(SEARCH-MI)。在此分析中,我们评估了从上次心肌梗死(MI)到预防性心脏复律除颤器(ICD)植入之间的时间间隔对设备激活的影响。
643 名左心室功能障碍(平均 LVEF 26±5%)和 NYHA Ⅰ-Ⅲ级的患者前瞻性地在多中心注册研究中随访了 1.8±1.2 年。根据上次 MI 和 ICD 植入之间的时间,将人群分为 3 组:[1]从 40 天到小于 1.5 年;[2]从 1.5 年到小于 7 年;[3]至少 7 年。
从上次 MI 到 ICD 植入时间较长的患者发生室性心动过速和适当的设备治疗(ATP 或电击)的累积发生率更高(Gray's Test p=0.002 和 p=0.013)。在 MI 分层组中,全因死亡率(Gray's Test p=0.618)或心源性猝死(Gray's Test p=0.663)均无显著差异。
MI 后植入 ICD 时间较长的患者发生室性心动过速和适当的 ICD 治疗的机会更高,而总死亡率无差异。这些观察结果对于改善预防猝死的患者目标定位可能很重要。