University of Toronto, Canada.
Peter Munk Cardiac Centre, University Health Network, Toronto, Ontario, Canada.
J Am Heart Assoc. 2017 Aug 19;6(8):e006220. doi: 10.1161/JAHA.117.006220.
We sought to examine the mortality impact of appropriate implantable cardioverter defibrillator (ICD) therapy between patients who received ICD for primary versus secondary prevention purposes.
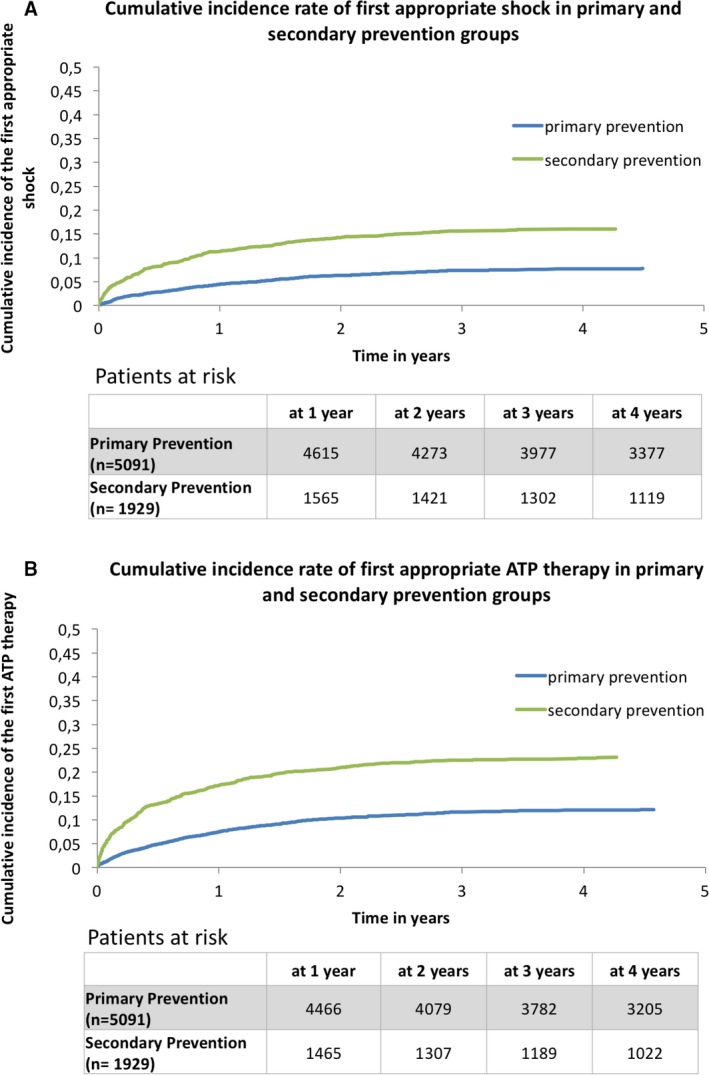
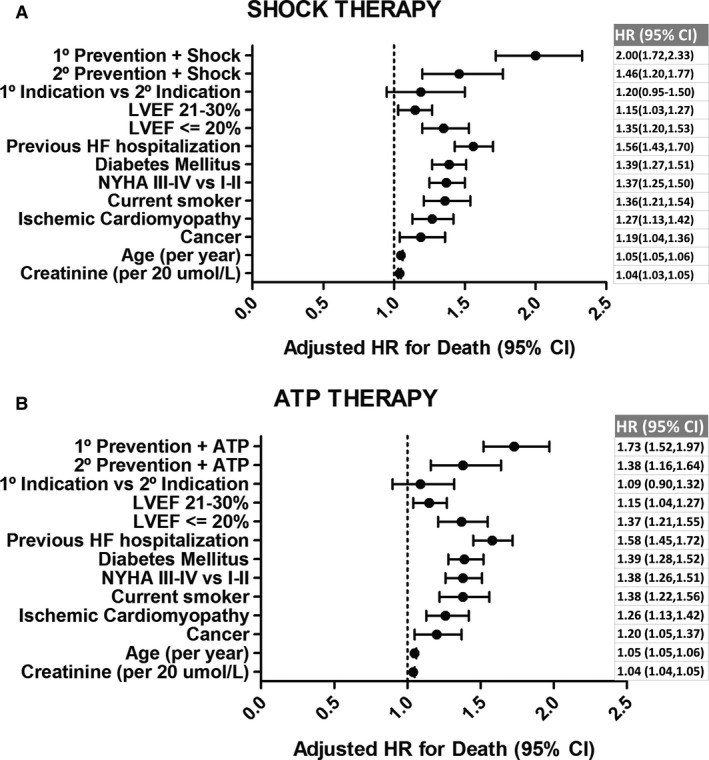
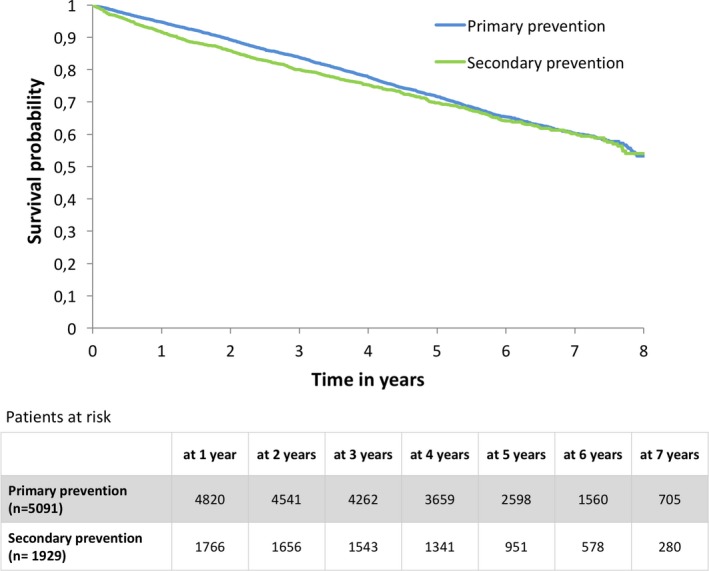
From a prospective, population-based registry, we identified 7020 patients who underwent de novo ICD implantation between February 2007 and May 2012 in Ontario, Canada. The primary outcome was all-cause mortality. We used multivariable Cox proportional hazard modeling to adjust for differences in baseline characteristics and analyzed the mortality impact of first appropriate ICD therapy (shock and antitachycardia pacing [ATP]) as a time-varying covariate. There were 1929 (27.5%) patients who received ICDs for secondary prevention purposes. The median follow-up period was 5.02 years. Compared with those with secondary prevention ICDs, patients with primary prevention ICDs had more medical comorbidities, and lower ejection fraction. Patients who experienced appropriate ICD shock or ATP had greater risk of death compared with those who did not, irrespective of implant indication. In the primary prevention group, the adjusted hazard ratios of death for appropriate shock and ATP were 2.00 (95% CI: 1.72-2.33) and 1.73 (95% CI: 1.52-1.97), respectively. In the secondary prevention group, the adjusted hazard ratios of death for appropriate ICD shock and ATP were 1.46 (95% CI: 1.20-1.77) and 1.38 (95% CI: 1.16-1.64), respectively.
Despite having a more favorable clinical profile, occurrence of appropriate ICD shock or ATP in patients with secondary prevention ICDs was associated with similar magnitudes of mortality risk as those with primary prevention ICDs. A heightened degree of care is warranted for all patients who experience appropriate ICD shock or ATP therapy.
我们旨在研究因一级预防和二级预防目的而植入植入式心律转复除颤器(ICD)的患者之间,恰当的 ICD 治疗对死亡率的影响。
我们从一个前瞻性的、基于人群的登记处中确定了 7020 例 2007 年 2 月至 2012 年 5 月期间在加拿大安大略省新植入 ICD 的患者。主要结局为全因死亡率。我们使用多变量 Cox 比例风险模型来调整基线特征的差异,并分析首次恰当 ICD 治疗(电击和抗心动过速起搏[ATP])作为时变协变量的死亡率影响。有 1929 例(27.5%)患者因二级预防目的而植入 ICD。中位随访期为 5.02 年。与因二级预防植入 ICD 的患者相比,因一级预防植入 ICD 的患者有更多的合并症,射血分数更低。经历过恰当 ICD 电击或 ATP 的患者与未经历过的患者相比,死亡风险更高,与植入指征无关。在一级预防组中,恰当电击和 ATP 的死亡调整后风险比分别为 2.00(95%CI:1.72-2.33)和 1.73(95%CI:1.52-1.97)。在二级预防组中,恰当 ICD 电击和 ATP 的死亡调整后风险比分别为 1.46(95%CI:1.20-1.77)和 1.38(95%CI:1.16-1.64)。
尽管二级预防 ICD 患者的临床状况更为有利,但经历恰当 ICD 电击或 ATP 与一级预防 ICD 患者的死亡率风险相当。所有经历恰当 ICD 电击或 ATP 治疗的患者都需要高度关注。