Division of Endocrinology and Metabolism, Department of Internal Medicine, Center for Thyroid Cancer, National Cancer Center, Goyang, Korea.
J Korean Med Sci. 2012 Sep;27(9):1014-8. doi: 10.3346/jkms.2012.27.9.1014. Epub 2012 Aug 22.
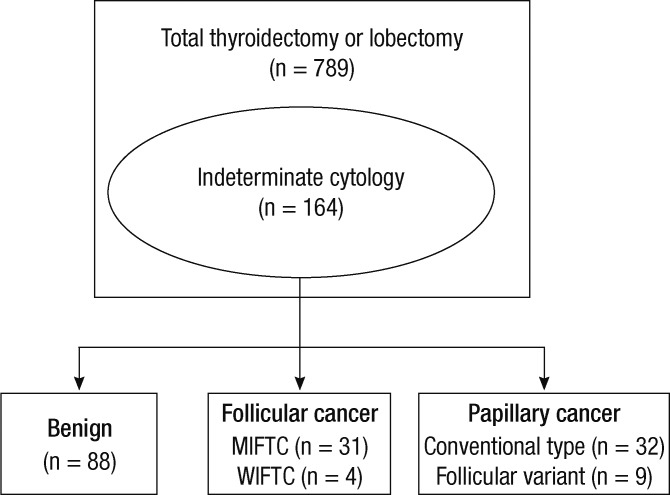
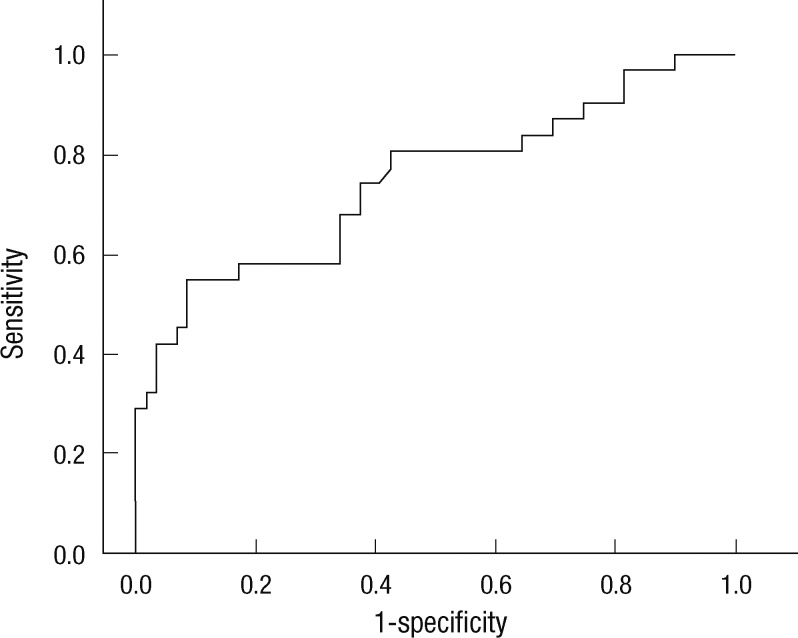
Indeterminate cytology results increase the number of repetitive procedure and unnecessary surgery. This study was designed to find useful and simple predictive tools to differentiate malignant thyroid nodules from indeterminate nodules. We retrospectively enrolled 164 patients who had undergone thyroid surgery as a result of indeterminate cytology in the National Cancer Center. We reviewed patients' age at diagnosis, sex, preoperative biochemical markers such as thyroglobulin (Tg), anti-Tg antibody, free T4 and TSH level, and sonographical and pathological findings, which were subjected to statistical analysis. We found several clinical and sonographical predictive factors that showed significant differences. Young age, male, preoperative high Tg level, and hypoechoic nodule on sonography all increased cancer probability significantly in multivariate analysis. With a cut-off value of 187.5 ng/mL Tg, sensitivity and specificity were 54.8% and 90.1%, respectively (AUC 0.748, P < 0.001). In the case of nodule size > 1.7 cm, elevated serum Tg predicts the risk of malignancy; especially Tg > 70 ng/mL (odds ratio 3.245, 95% confidence interval 1.115-9.450, P = 0.038). Preoperative Tg levels had very high specificity in predicting thyroid cancer in case of suspicious follicular neoplasm. Therefore, Tg levels may be a useful marker for differentiating thyroid cancer from benign thyroid nodules in the cytological diagnosis of indeterminate nodules.
不确定的细胞学结果会增加重复操作和不必要手术的数量。本研究旨在寻找有用且简单的预测工具,以区分恶性甲状腺结节和不确定的结节。我们回顾性地招募了 164 名因不确定的细胞学结果而在国家癌症中心接受甲状腺手术的患者。我们回顾了患者的诊断年龄、性别、术前生化标志物,如甲状腺球蛋白(Tg)、抗 Tg 抗体、游离 T4 和 TSH 水平,以及超声和病理发现,并进行了统计学分析。我们发现了一些具有显著差异的临床和超声预测因素。多变量分析显示,年轻、男性、术前高 Tg 水平和超声下低回声结节均显著增加癌症的可能性。当 Tg 截值为 187.5ng/mL 时,敏感性和特异性分别为 54.8%和 90.1%(AUC 为 0.748,P<0.001)。对于结节大小>1.7cm 的情况,血清 Tg 升高预测恶性风险;特别是 Tg>70ng/mL(比值比 3.245,95%置信区间 1.115-9.450,P=0.038)。在可疑滤泡性肿瘤的情况下,术前 Tg 水平对预测甲状腺癌具有非常高的特异性。因此,Tg 水平可能是区分甲状腺癌和不确定结节中的良性甲状腺结节的有用标志物。