San Raffaele Telethon Institute for Gene Therapy Milan, Italy.
Front Immunol. 2012 Aug 27;3:265. doi: 10.3389/fimmu.2012.00265. eCollection 2012.
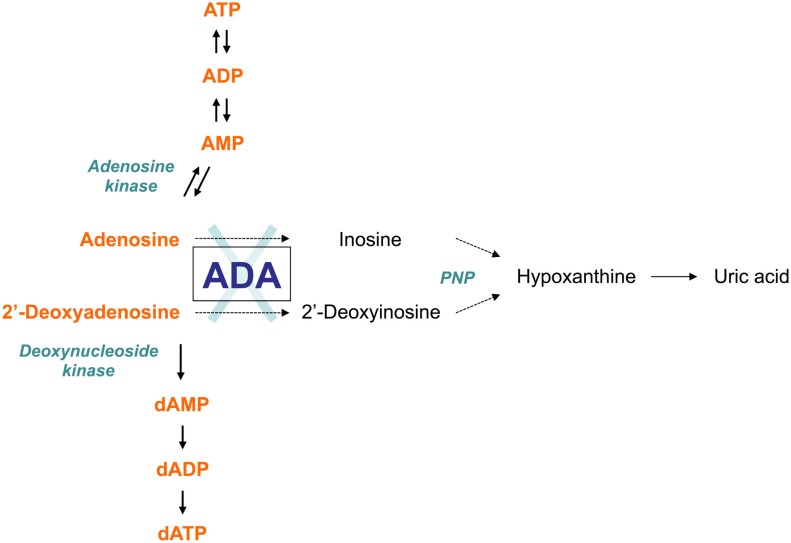
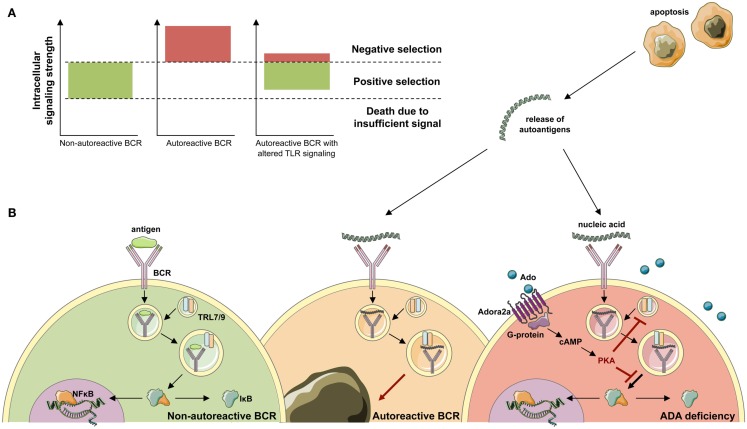
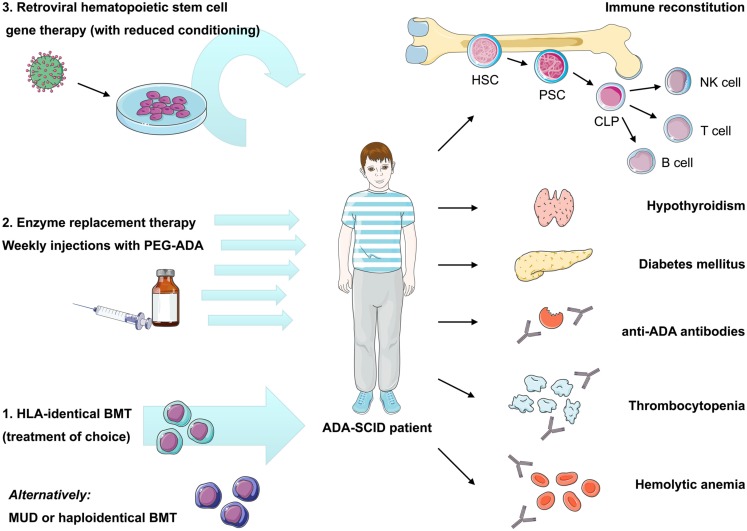
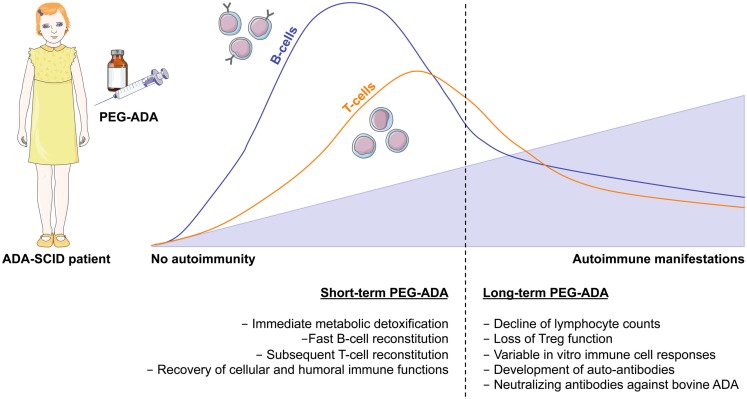
Genetic defects in the adenosine deaminase (ADA) gene are among the most common causes for severe combined immunodeficiency (SCID). ADA-SCID patients suffer from lymphopenia, severely impaired cellular and humoral immunity, failure to thrive, and recurrent infections. Currently available therapeutic options for this otherwise fatal disorder include bone marrow transplantation (BMT), enzyme replacement therapy with bovine ADA (PEG-ADA), or hematopoietic stem cell gene therapy (HSC-GT). Although varying degrees of immune reconstitution can be achieved by these treatments, breakdown of tolerance is a major concern in ADA-SCID. Immune dysregulation such as autoimmune hypothyroidism, diabetes mellitus, hemolytic anemia, and immune thrombocytopenia are frequently observed in milder forms of the disease. However, several reports document similar complications also in patients on long-term PEG-ADA and after BMT or GT treatment. A skewed repertoire and decreased immune functions have been implicated in autoimmunity observed in certain B-cell and/or T-cell immunodeficiencies, but it remains unclear to what extent specific mechanisms of tolerance are affected in ADA deficiency. Herein we provide an overview about ADA-SCID and the autoimmune manifestations reported in these patients before and after treatment. We also assess the value of the ADA-deficient mouse model as a useful tool to study both immune and metabolic disease mechanisms. With focus on regulatory T- and B-cells we discuss the lymphocyte subpopulations particularly prone to contribute to the loss of self-tolerance and onset of autoimmunity in ADA deficiency. Moreover we address which aspects of immune dysregulation are specifically related to alterations in purine metabolism caused by the lack of ADA and the subsequent accumulation of metabolites with immunomodulatory properties.
腺苷脱氨酶(ADA)基因的遗传缺陷是严重联合免疫缺陷(SCID)最常见的原因之一。ADA-SCID 患者会出现淋巴细胞减少症、严重的细胞和体液免疫缺陷、生长不良和反复感染。目前,这种致命疾病的治疗选择包括骨髓移植(BMT)、牛 ADA(PEG-ADA)酶替代疗法或造血干细胞基因疗法(HSC-GT)。尽管这些治疗方法可以在不同程度上实现免疫重建,但在 ADA-SCID 中,耐受的破坏是一个主要问题。免疫失调,如自身免疫性甲状腺功能减退、糖尿病、溶血性贫血和免疫性血小板减少症,在疾病的较轻形式中经常观察到。然而,有几个报告记录了在接受长期 PEG-ADA 以及 BMT 或 GT 治疗的患者中也存在类似的并发症。在某些 B 细胞和/或 T 细胞免疫缺陷中,观察到自身免疫与偏倚的 repertoire 和免疫功能下降有关,但在 ADA 缺乏中,特定的耐受机制受到影响的程度仍不清楚。在此,我们提供了 ADA-SCID 的概述以及这些患者在治疗前后报告的自身免疫表现。我们还评估了 ADA 缺陷小鼠模型作为研究免疫和代谢疾病机制的有用工具的价值。我们重点关注调节性 T 细胞和 B 细胞,讨论特别容易导致 ADA 缺乏中自身耐受性丧失和自身免疫发作的淋巴细胞亚群。此外,我们还探讨了哪些免疫失调方面与缺乏 ADA 引起的嘌呤代谢改变以及随后具有免疫调节特性的代谢物的积累有关。