Griffiths Robert I, Gleeson Michelle L, Mikhael Joseph, Danese Mark D
Outcomes Insights Inc., 340 N. Westlake Boulevard, Suite 200, Westlake Village, CA 91362, USA.
J Cancer Epidemiol. 2012;2012:978391. doi: 10.1155/2012/978391. Epub 2012 Aug 27.
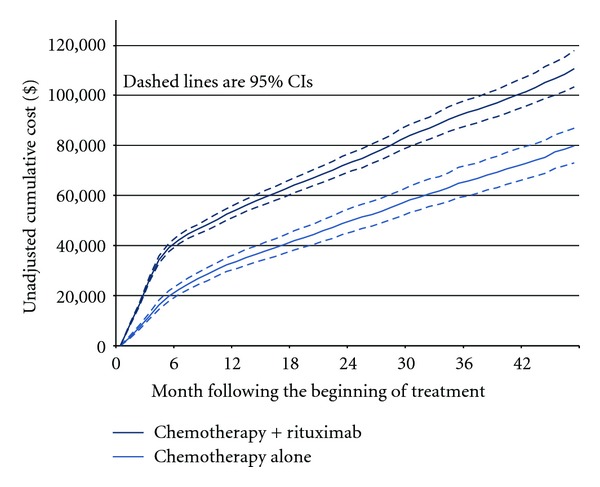
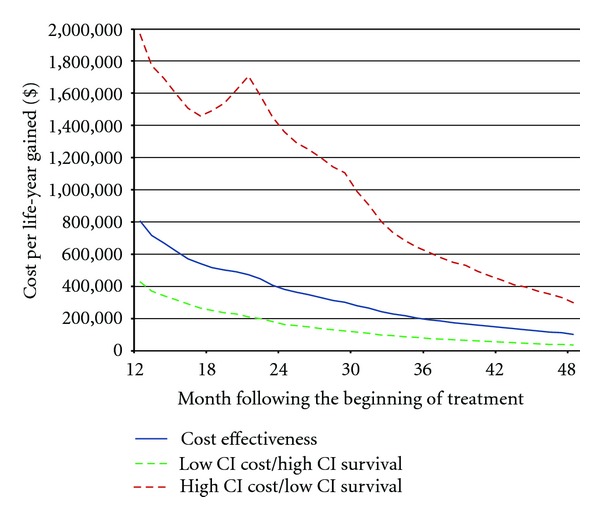
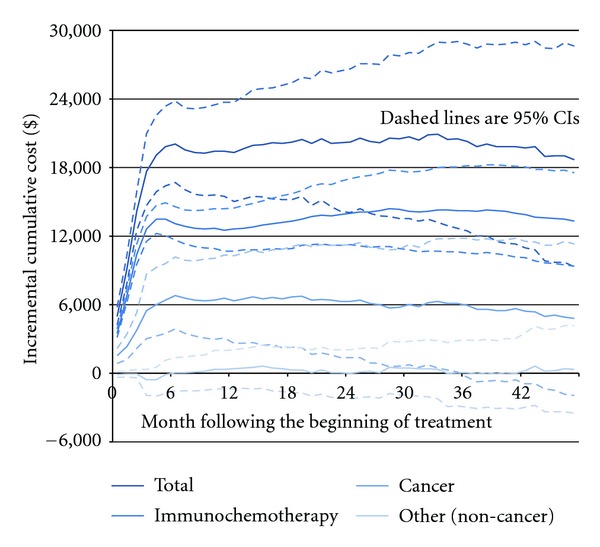
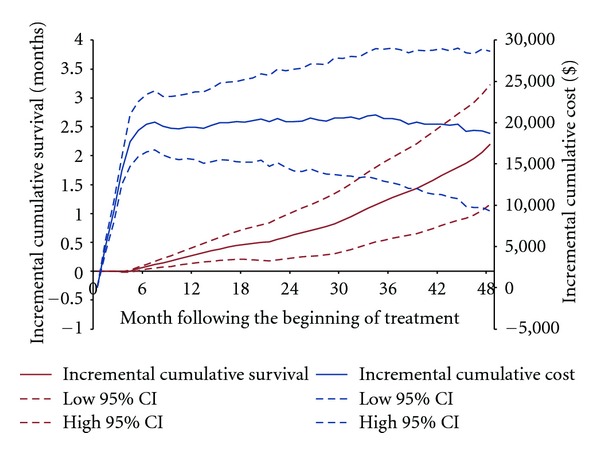
Rituximab improves survival in follicular lymphoma (FL), but is considerably more expensive than conventional chemotherapy. We estimated the total direct medical costs, cumulative survival, and cost-effectiveness of adding rituximab to first-line chemotherapy for FL, based on a single source of data representing routine practice in the elderly. Using surveillance, epidemiology, and end results (SEER) registry data plus Medicare claims, we identified 1,117 FL patients who received first-line CHOP (cyclophosphamide (C), doxorubicin, vincristine (V), and prednisone (P)) or CVP +/- rituximab. Multivariate regression was used to estimate adjusted cumulative cost and survival differences between the two groups over four years after beginning treatment. The median age was 73 years (minimum 66 years), 56% had stage III-IV disease, and 67% received rituximab. Adding rituximab to first-line chemotherapy was associated with higher adjusted incremental total cost ($18,695; 95% Confidence Interval (CI) $9,302-$28,643) and longer adjusted cumulative survival (0.18 years; 95% CI 0.10-0.27) over four years of followup. The expected cost-effectiveness was $102,142 (95% CI $34,531-296,337) per life-year gained. In routine clinical practice, adding rituximab to first-line chemotherapy for elderly patients with FL results in higher direct medical costs to Medicare and longer cumulative survival after four years.
利妥昔单抗可提高滤泡性淋巴瘤(FL)患者的生存率,但比传统化疗昂贵得多。我们基于单一来源的代表老年人常规医疗的数据,估算了在FL一线化疗中添加利妥昔单抗的总直接医疗成本、累积生存率和成本效益。利用监测、流行病学和最终结果(SEER)登记数据以及医疗保险理赔数据,我们识别出1117例接受一线CHOP(环磷酰胺(C)、阿霉素、长春新碱(V)和泼尼松(P))或CVP±利妥昔单抗治疗的FL患者。使用多变量回归来估算两组在开始治疗后四年内调整后的累积成本和生存差异。中位年龄为73岁(最小66岁),56%的患者为III-IV期疾病,67%的患者接受了利妥昔单抗治疗。在一线化疗中添加利妥昔单抗与更高的调整后增量总成本(18,695美元;95%置信区间(CI)9,302美元至28,643美元)以及四年随访期间更长的调整后累积生存期(0.18年;95%CI 0.10至0.27)相关。每获得一个生命年的预期成本效益为102,142美元(95%CI 34,531美元至296,337美元)。在常规临床实践中,对于老年FL患者,在一线化疗中添加利妥昔单抗会导致医疗保险的直接医疗成本增加,且四年后的累积生存期更长。