Research Unit of Clinical Epidemiology, Institute of Clinical Research, University of Southern Denmark, Odense, Denmark.
BMC Med Res Methodol. 2012 Sep 12;12:139. doi: 10.1186/1471-2288-12-139.
Information from blood cultures is utilized for infection control, public health surveillance, and clinical outcome research. This information can be enriched by physicians' assessments of positive blood cultures, which are, however, often available from selected patient groups or pathogens only. The aim of this work was to determine whether patients with positive blood cultures can be classified effectively for outcome research in epidemiological studies by the use of administrative data and computer algorithms, taking physicians' assessments as reference.
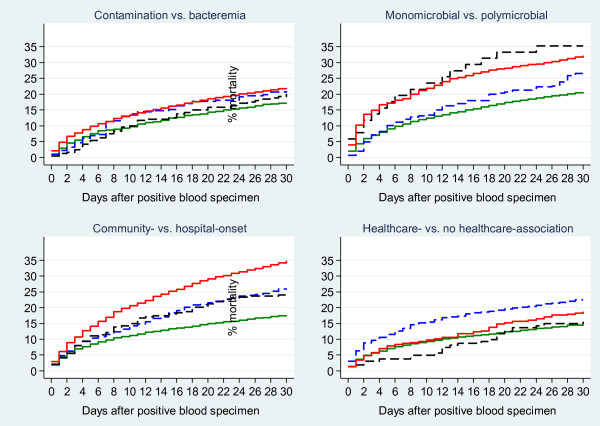
Physicians' assessments of positive blood cultures were routinely recorded at two Danish hospitals from 2006 through 2008. The physicians' assessments classified positive blood cultures as: a) contamination or bloodstream infection; b) bloodstream infection as mono- or polymicrobial; c) bloodstream infection as community- or hospital-onset; d) community-onset bloodstream infection as healthcare-associated or not. We applied the computer algorithms to data from laboratory databases and the Danish National Patient Registry to classify the same groups and compared these with the physicians' assessments as reference episodes. For each classification, we tabulated episodes derived by the physicians' assessment and the computer algorithm and compared 30-day mortality between concordant and discrepant groups with adjustment for age, gender, and comorbidity.
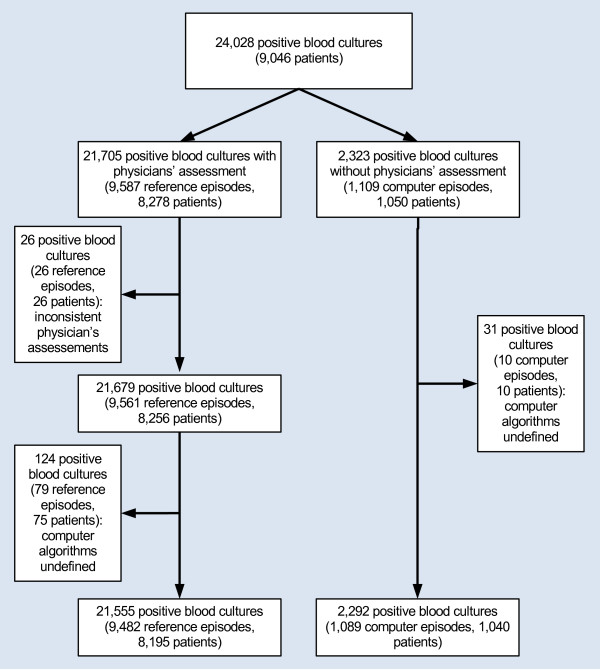
Physicians derived 9,482 reference episodes from 21,705 positive blood cultures. The agreement between computer algorithms and physicians' assessments was high for contamination vs. bloodstream infection (8,966/9,482 reference episodes [96.6%], Kappa = 0.83) and mono- vs. polymicrobial bloodstream infection (6,932/7,288 reference episodes [95.2%], Kappa = 0.76), but lower for community- vs. hospital-onset bloodstream infection (6,056/7,288 reference episodes [83.1%], Kappa = 0.57) and healthcare-association (3,032/4,740 reference episodes [64.0%], Kappa = 0.15). The 30-day mortality in the discrepant groups differed from the concordant groups as regards community- vs. hospital-onset, whereas there were no material differences within the other comparison groups.
Using data from health administrative registries, we found high agreement between the computer algorithms and the physicians' assessments as regards contamination vs. bloodstream infection and monomicrobial vs. polymicrobial bloodstream infection, whereas there was only moderate agreement between the computer algorithms and the physicians' assessments concerning the place of onset. These results provide new information on the utility of computer algorithms derived from health administrative registries.
血液培养物的信息可用于感染控制、公共卫生监测和临床结果研究。然而,这些信息可以通过医生对阳性血培养物的评估来丰富,而这些评估通常仅来自于选定的患者群体或病原体。本研究的目的是确定是否可以通过使用行政数据和计算机算法,根据医生的评估对阳性血培养物患者进行有效的分类,以用于流行病学研究中的结果研究,并将其作为参考。
2006 年至 2008 年,在丹麦的两家医院常规记录医生对阳性血培养物的评估。医生的评估将阳性血培养物分类为:a)污染或血流感染;b)血流感染为单一或多种微生物;c)血流感染为社区或医院发病;d)社区发病的血流感染与医疗保健相关或不相关。我们将计算机算法应用于实验室数据库和丹麦国家患者登记处的数据,以对相同的组进行分类,并将其与医生的评估作为参考病例进行比较。对于每种分类,我们列出了医生评估和计算机算法得出的病例,并比较了 30 天死亡率在一致和不一致组之间的差异,并调整了年龄、性别和合并症。
医生从 21,705 份阳性血培养物中得出了 9,482 份参考病例。计算机算法与医生评估之间的一致性很高,污染与血流感染(8,966/9,482 参考病例[96.6%],Kappa=0.83)和单一与多种微生物血流感染(6,932/7,288 参考病例[95.2%],Kappa=0.76),但社区与医院发病的血流感染(6,056/7,288 参考病例[83.1%],Kappa=0.57)和医疗保健相关(3,032/4,740 参考病例[64.0%],Kappa=0.15)的一致性较低。不一致组的 30 天死亡率与一致组不同,涉及社区与医院发病,而在其他比较组中没有明显差异。
使用健康行政登记处的数据,我们发现计算机算法与医生评估之间在污染与血流感染以及单一与多种微生物血流感染方面的一致性很高,而在发病地点方面,计算机算法与医生评估之间的一致性仅为中等。这些结果提供了有关从健康行政登记处获得的计算机算法的实用性的新信息。