Dewitte Antoine, Coquin Julien, Meyssignac Bertrand, Joannès-Boyau Olivier, Fleureau Catherine, Roze Hadrien, Ripoche Jean, Janvier Gérard, Combe Christian, Ouattara Alexandre
Crit Care. 2012 Sep 12;16(5):R165. doi: 10.1186/cc11517.
Renal resistive index (RI), determined by Doppler ultrasonography, directly reveals and quantifies modifications in renal vascular resistance. The aim of this study was to evaluate if mean arterial pressure (MAP) is determinant of renal RI in septic, critically ill patients suffering or not from acute kidney injury (AKI).
This prospective observational study included 96 patients. AKI was defined according to RIFLE criteria and transient or persistent AKI according to renal recovery within 3 days.
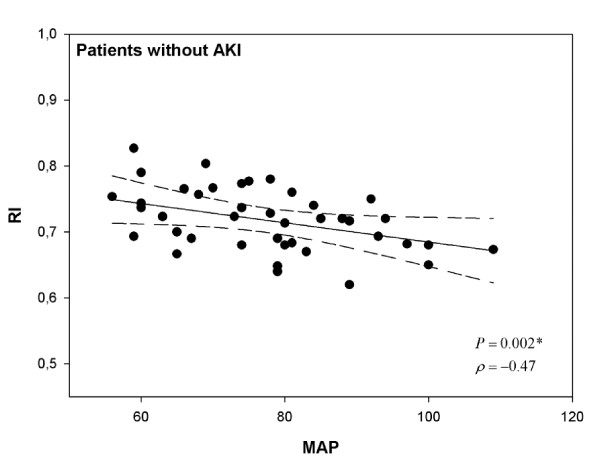
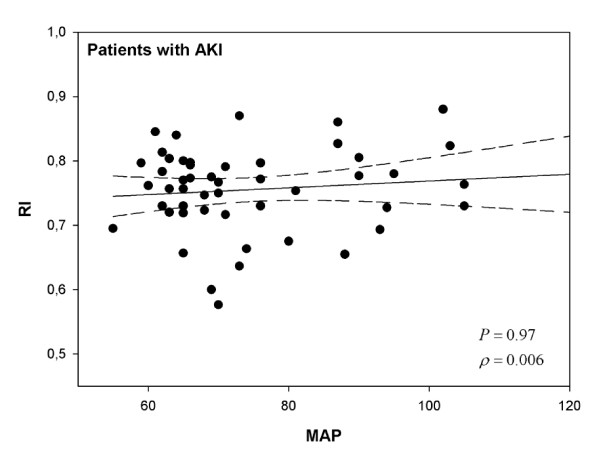
Median renal RIs were 0.72 (0.68-0.75) in patients without AKI and 0.76 (0.72-0.80) in patients with AKI (P = 0.001). RIs were 0.75 (0.72-0.79) in transient AKI and 0.77 (0.70-0.80) in persistent AKI (P = 0.84). RI did not differ in patients given norepinephrine infusion and was not correlated with norepinephrine dose. RI was correlated with MAP (ρ = -0.47; P = 0.002), PaO2/FiO2 ratio (ρ = -0.33; P = 0.04) and age (ρ = 0.35; P = 0.015) only in patients without AKI.
A poor correlation between renal RI and MAP, age, or PaO2/FiO2 ratio was found in septic and critically ill patients without AKI compared to patients with AKI. These findings suggest that determinants of RI are multiple. Renal circulatory response to sepsis estimated by Doppler ultrasonography cannot reliably be predicted simply from changes in systemic hemodynamics. As many factors influence its value, the interest in a single RI measurement at ICU admission to determine optimal MAP remains uncertain.
通过多普勒超声测定的肾阻力指数(RI)可直接显示并量化肾血管阻力的变化。本研究的目的是评估平均动脉压(MAP)是否为脓毒症、患有或未患有急性肾损伤(AKI)的重症患者肾RI的决定因素。
这项前瞻性观察性研究纳入了96例患者。根据RIFLE标准定义AKI,并根据3天内的肾功能恢复情况定义短暂性或持续性AKI。
无AKI患者的肾RI中位数为0.72(0.68 - 0.75),有AKI患者为0.76(0.72 - 0.80)(P = 0.001)。短暂性AKI患者的RI为0.75(0.72 - 0.79),持续性AKI患者为0.77(0.70 - 0.80)(P = 0.84)。接受去甲肾上腺素输注的患者RI无差异,且与去甲肾上腺素剂量无关。仅在无AKI的患者中,RI与MAP(ρ = -0.47;P = 0.002)、PaO2/FiO2比值(ρ = -0.33;P = 0.04)和年龄(ρ = 0.35;P = 0.015)相关。
与患有AKI的患者相比,在无AKI的脓毒症和重症患者中,发现肾RI与MAP、年龄或PaO2/FiO2比值之间的相关性较差。这些发现表明RI的决定因素是多方面的。通过多普勒超声评估的肾循环对脓毒症的反应不能仅根据全身血流动力学的变化可靠地预测。由于许多因素影响其值,在重症监护病房入院时单次测量RI以确定最佳MAP的意义仍不确定。