Department of Molecular Medicine, Aarhus University Hospital, Skejby, Denmark.
Br J Cancer. 2012 Oct 9;107(8):1392-8. doi: 10.1038/bjc.2012.412. Epub 2012 Sep 13.
Multiple clinical risk factors and genetic profiles have been demonstrated to predict progression of non-muscle invasive bladder cancer; however, no easily clinical applicable gene signature has been developed to predict disease progression independent of disease stage and grade.
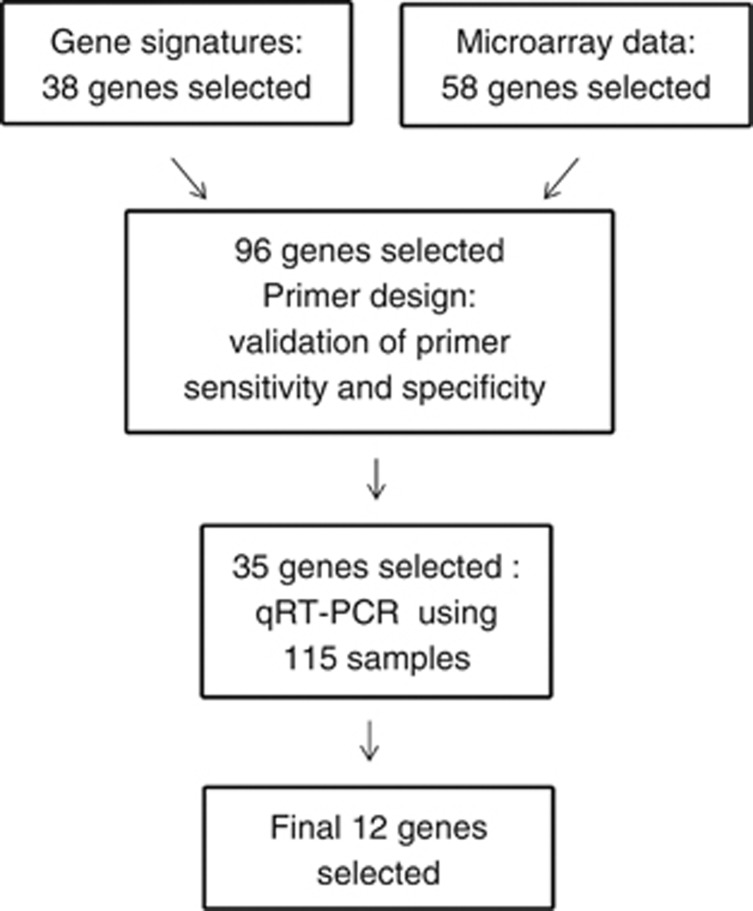
We measured the intra-patient variation of an 88-gene progression signature using 39 metachronous tumours from 17 patients. For delineation of the optimal quantitative reverse transcriptase PCR panel of markers, we used 115 tumour samples from patients in Denmark, Sweden, UK and Spain.
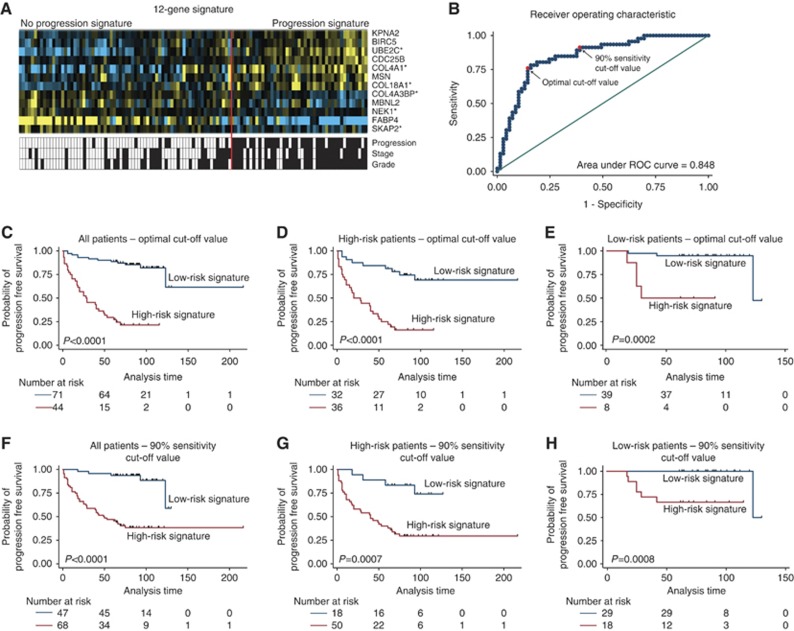
Analysis of intra-patient variation of the molecular markers showed 71% similar classification results. A final panel of 12 genes was selected, showing significant correlation with outcome. In multivariate Cox regression analysis, we found that the 12-gene signature was an independent prognostic factor (hazard ratio=7.4 (95% confidence interval: 3.4-15.9), P<0.001) when adjusting for stage, grade and treatment. Independent validation of the 12-gene panel and the determined cut-off values is needed and ongoing.
Intra-patient marker variation in metachronous tumours is present. Therefore, to increase test sensitivity, it may be necessary to test several metachronous tumours from a patient's disease course. A PCR-based 12-gene signature significantly predicts disease progression in patients with non-muscle invasive bladder cancer.
多项临床风险因素和基因谱已被证明可预测非肌肉浸润性膀胱癌的进展;然而,目前还没有一种易于临床应用的基因特征可以独立于疾病分期和分级来预测疾病进展。
我们使用 17 名患者的 39 个异时性肿瘤测量了 88 个进展特征基因的患者内变异。为了确定最佳的定量逆转录酶聚合酶链反应(PCR)标记物定量检测面板,我们使用了来自丹麦、瑞典、英国和西班牙的 115 名患者的肿瘤样本。
对分子标记物的患者内变异分析显示 71%具有相似的分类结果。最终选择了一个由 12 个基因组成的面板,该面板与结果显著相关。在多变量 Cox 回归分析中,我们发现 12 基因特征是独立的预后因素(危险比=7.4(95%置信区间:3.4-15.9),P<0.001),在调整分期、分级和治疗后。需要并正在对 12 基因面板和确定的截断值进行独立验证。
异时性肿瘤中的患者内标记物变异存在。因此,为了提高测试的灵敏度,可能需要测试患者疾病过程中的多个异时性肿瘤。基于 PCR 的 12 基因特征可显著预测非肌肉浸润性膀胱癌患者的疾病进展。