Rim Chai Hong, Yang Dae Sik, Park Young Je, Yoon Won Sup, Lee Jung Ae, Kim Chul Yong
Department of Radiation Oncology, Korea University Medical Center, Seoul, Korea.
Radiat Oncol J. 2011 Sep;29(3):156-63. doi: 10.3857/roj.2011.29.3.156. Epub 2011 Sep 30.
To evaluate long-term local control rate and toxicity in patients treated with external beam radiotherapy (EBRT) for pituitary adenomas.
We retrospectively reviewed the medical records of 60 patients treated with EBRT for pituitary adenoma at Korea University Medical Center from 1996 and 2006. Thirty-five patients had hormone secreting tumors, 25 patients had non-secreting tumors. Fifty-seven patients had received postoperative radiotherapy (RT), and 3 had received RT alone. Median total dose was 54 Gy (range, 36 to 61.2 Gy). The definition of tumor progression were as follows: evidence of tumor progression on computed tomography or magnetic resonance imaging, worsening of clinical sign requiring additional operation or others, rising serum hormone level against a previously stable or falling value, and failure of controlling serum hormone level so that the hormone level had been far from optimal range until last follow-up. Age, sex, hormone secretion, tumor extension, tumor size, and radiation dose were analyzed for prognostic significance in tumor control.
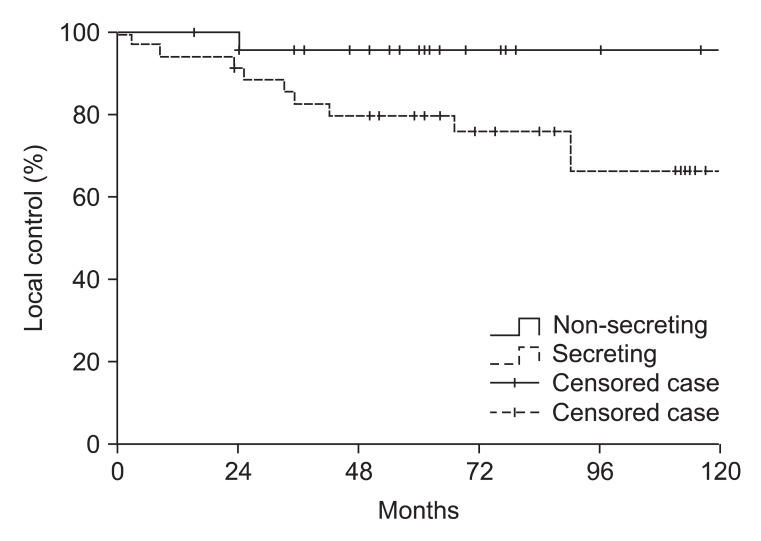
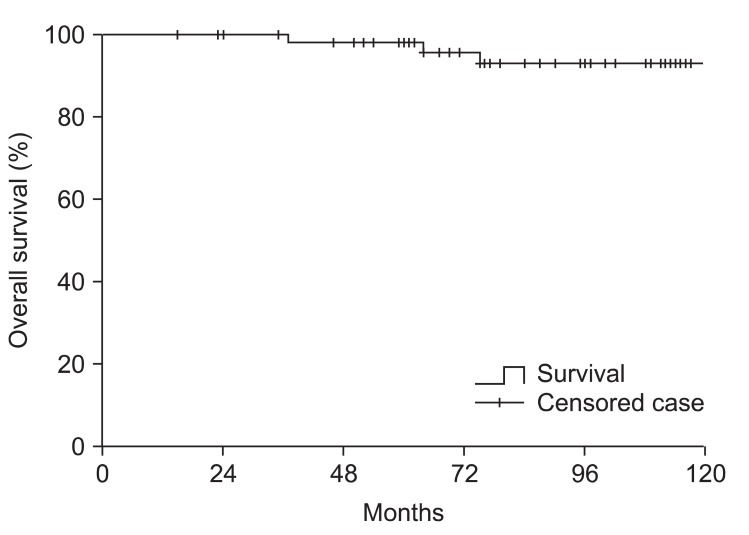
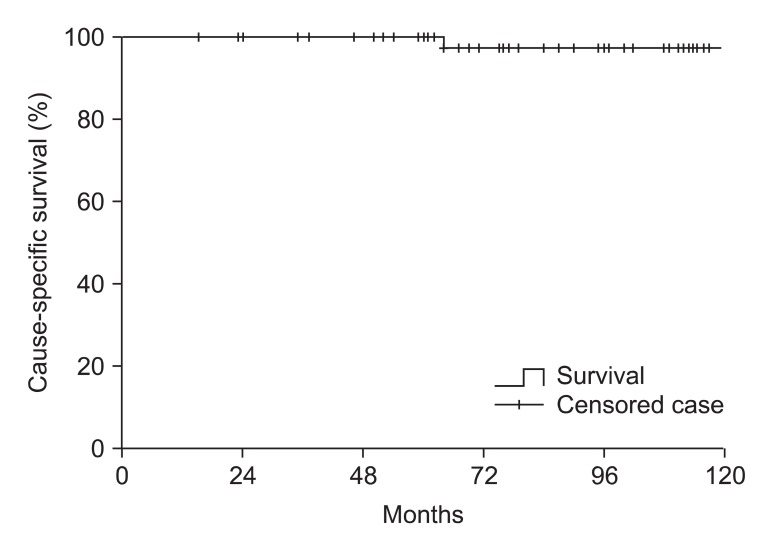
Median follow-up was 5.7 years (range, 2 to 14.4 years). The 10-year actuarial local control rates for non-secreting and secreting adenomas were 96% and 66%, respectively. In univariate analysis, hormone secretion was significant prognostic factor (p = 0.042) and cavernous sinus extension was marginally significant factor (p = 0.054) for adverse local control. All other factors were not significant. In multivariate analysis, hormone secretion and gender were significant. Fifty-three patients had mass-effect symptoms (headache, dizziness, visual disturbance, hypopituitarism, loss of consciousness, and cranial nerve palsy). A total of 17 of 23 patients with headache and 27 of 34 patients with visual impairment were improved. Twenty-seven patients experienced symptoms of endocrine hypersecretion (galactorrhea, amenorrhea, irregular menstruation, decreased libido, gynecomastia, acromegaly, and Cushing's disease). Amenorrhea was abated in 7 of 10 patients, galactorrhea in 8 of 8 patients, acromegaly in 7 of 11 patients, Cushing's disease in 4 of 4 patients. Long-term complication was observed in 4 patients; 3 patients with cerebrovascular accident, 1 patient developed dementia. Of these patients, 3 of 4 received more than 60 Gy of irradiation.
EBRT is highly effective in preventing recurrence and reducing mass effect of non-secreting adenoma. Effort to improve tumor control of secreting adenoma is required. Careful long-term follow-up is required when relatively high dose is applied. Modern radiosurgery or proton RT may be options to decrease late complications.
评估接受垂体腺瘤外照射放疗(EBRT)患者的长期局部控制率和毒性。
我们回顾性分析了1996年至2006年在韩国大学医学中心接受EBRT治疗的60例垂体腺瘤患者的病历。35例患者患有分泌激素肿瘤,25例患者患有无分泌功能肿瘤。57例患者接受了术后放疗(RT),3例患者仅接受了RT。中位总剂量为54 Gy(范围为36至61.2 Gy)。肿瘤进展的定义如下:计算机断层扫描或磁共振成像显示肿瘤进展的证据、临床症状恶化需要额外手术或其他治疗、血清激素水平相对于先前稳定或下降的值上升、以及未能控制血清激素水平以至于直到最后一次随访时激素水平一直远离最佳范围。分析年龄、性别、激素分泌、肿瘤扩展、肿瘤大小和放射剂量对肿瘤控制的预后意义。
中位随访时间为5.7年(范围为2至14.4年)。无分泌功能腺瘤和分泌功能腺瘤的10年精算局部控制率分别为96%和66%。在单因素分析中,激素分泌是局部控制不良的显著预后因素(p = 0.042),海绵窦扩展是边缘显著因素(p = 0.054)。所有其他因素均不显著。在多因素分析中,激素分泌和性别显著。53例患者有占位效应症状(头痛、头晕、视力障碍、垂体功能减退、意识丧失和颅神经麻痹)。23例头痛患者中的17例和34例视力障碍患者中的27例症状得到改善。27例患者有内分泌功能亢进症状(溢乳、闭经、月经不调、性欲减退、男性乳房发育、肢端肥大症和库欣病)。10例闭经患者中的7例、8例溢乳患者中的8例、11例肢端肥大症患者中的7例、4例库欣病患者中的4例症状减轻。4例患者观察到长期并发症;3例患者发生脑血管意外,1例患者患痴呆症。在这些患者中,4例患者中有3例接受了超过60 Gy的照射。
EBRT在预防无分泌功能腺瘤复发和减轻占位效应方面非常有效。需要努力改善分泌功能腺瘤的肿瘤控制。当应用相对高剂量时,需要仔细的长期随访。现代放射外科或质子放疗可能是减少晚期并发症的选择。