Park Hyeli, Kim Ja Young, Lee Bo Mi, Chang Sei Kyung, Ko Seung Young, Kim Sung Jun, Park Dong Soo, Shin Hyun Soo
Department of Radiation Oncology, CHA Bundang Medical Center, CHA University, Seougnam, Korea.
Radiat Oncol J. 2011 Sep;29(3):199-205. doi: 10.3857/roj.2011.29.3.199. Epub 2011 Sep 30.
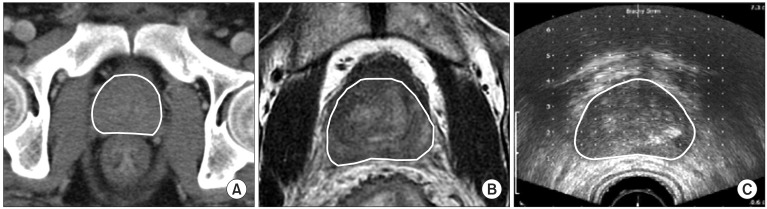
The present study compared the difference between intraoperative transrectal ultrasound (iTRUS)-based prostate volume and preplan computed tomography (CT), preplan magnetic resonance imaging (MRI)-based prostate volume to estimate the number of seeds needed for appropriate dose coverage in permanent brachytherapy for prostate cancer.
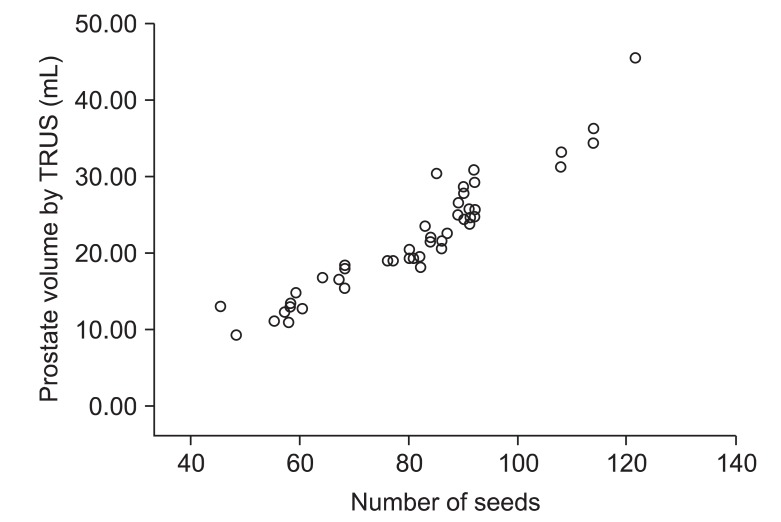
Between March 2007 and March 2011, among 112 patients who underwent permanent brachytherapy with (125)I, 60 image scans of 56 patients who underwent preplan CT (pCT) or preplan MRI (pMRI) within 2 months before brachytherapy were retrospectively reviewed. Twenty-four cases among 30 cases with pCT and 26 cases among 30 cases with pMRI received neoadjuvant hormone therapy (NHT). In 34 cases, NHT started after acquisition of preplan image. The median duration of NHT after preplan image acquisition was 17 and 21 days for cases with pCT and pMRI, respectively. The prostate volume calculated by different modalities was compared. And retrospective planning with iTRUS image was performed to estimate the number of (125)I seed required to obtain recommended dose distribution according to prostate volume.
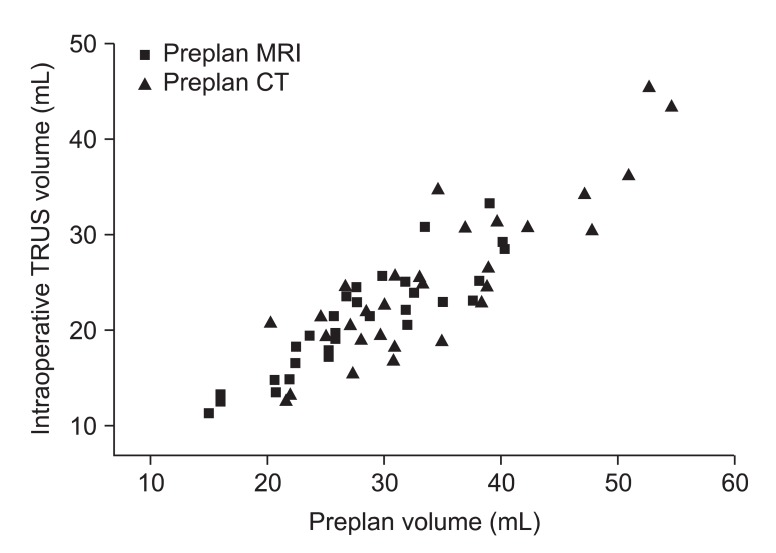
The mean difference in prostate volume was 9.05 mL between the pCT and iTRUS and 6.84 mL between the pMRI and iTRUS. The prostate volume was roughly overestimated by 1.36 times with pCT and by 1.33 times with pMRI. For 34 cases which received NHT after image acquisition, the prostate volume was roughly overestimated by 1.45 times with pCT and by 1.37 times with pMRI. A statistically significant difference was found between preplan image-based volume and iTRUS-based volume (p < 0.001). The median number of wasted seeds is approximately 13, when the pCT or pMRI volume was accepted without modification to assess the required number of seeds for brachytherapy.
pCT-based volume and pMRI-based volume tended to overestimate prostate volume in comparison to iTRUS-based volume. To reduce wasted seeds and cost of the brachytherapy, we should take the volume discrepancy into account when we estimate the number of (125)I seeds for permanent brachytherapy.
本研究比较了基于术中经直肠超声(iTRUS)的前列腺体积与计划前计算机断层扫描(CT)、计划前磁共振成像(MRI)的前列腺体积之间的差异,以估计前列腺癌永久性近距离放射治疗中实现适当剂量覆盖所需的粒子数量。
在2007年3月至2011年3月期间,对112例行¹²⁵I永久性近距离放射治疗的患者进行回顾性分析,其中56例患者在近距离放射治疗前2个月内进行了计划前CT(pCT)或计划前MRI(pMRI)扫描,共60次影像扫描。30例pCT患者中有24例、30例pMRI患者中有26例接受了新辅助激素治疗(NHT)。34例患者在获取计划前影像后开始NHT。对于pCT和pMRI患者,获取计划前影像后NHT的中位持续时间分别为17天和21天。比较了不同方法计算的前列腺体积。并利用iTRUS影像进行回顾性计划,以根据前列腺体积估计获得推荐剂量分布所需的¹²⁵I粒子数量。
pCT与iTRUS之间前列腺体积的平均差异为9.05 mL,pMRI与iTRUS之间为6.84 mL。pCT对前列腺体积的高估约为1.36倍,pMRI为1.33倍。对于34例在影像获取后接受NHT的患者,pCT对前列腺体积的高估约为1.45倍,pMRI为1.37倍。基于计划前影像的体积与基于iTRUS的体积之间存在统计学显著差异(p < 0.001)。当直接采用pCT或pMRI体积来评估近距离放射治疗所需的粒子数量时,浪费粒子的中位数约为13个。
与基于iTRUS的体积相比,基于pCT的体积和基于pMRI的体积往往会高估前列腺体积。为减少近距离放射治疗中浪费的粒子和成本,在估计¹²⁵I永久性近距离放射治疗的粒子数量时,应考虑体积差异。