National Center on Birth Defects and Developmental Disabilities, Centers for Disease Control and Prevention, 1600 Clifton Rd, MS-D02, Atlanta, GA 30329, USA.
Pediatrics. 2012 Oct;130(4):e812-20. doi: 10.1542/peds.2012-0267. Epub 2012 Sep 17.
Information on trends in venous thromboembolism (VTE) in US children is scant and inconsistent. We assessed national trends in VTE-associated pediatric hospitalizations.
All nonroutine newborn hospitalizations for children 0 to 17 years of age in the 1994-2009 Nationwide Inpatient Samples were included; routine newborn discharges were excluded. VTE diagnoses were identified by using the International Classification of Diseases, Ninth Revision, Clinical Modification codes. Variance weighted least square regression was used to assess trends in patient characteristics and rates of hospitalization per 100000 population <18 years of age. Multivariable logistic regression models were used to estimate the probability of VTE diagnosis over the study period.
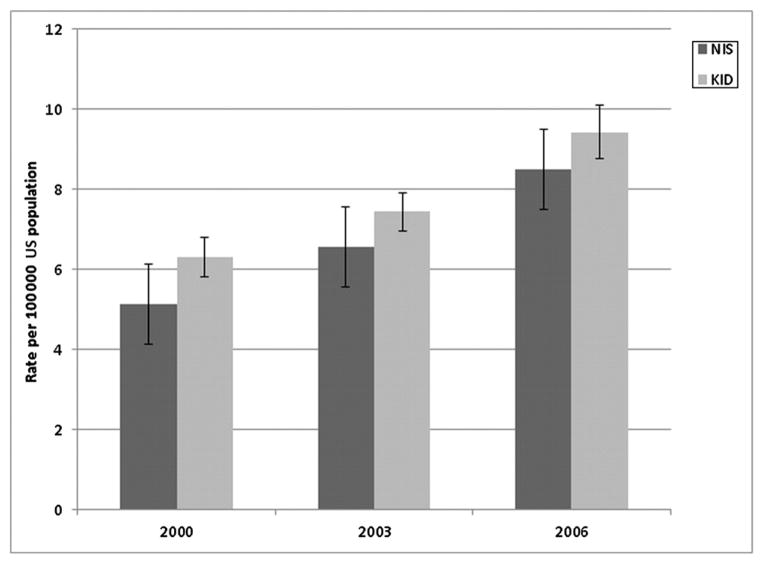
The rate of VTE-associated hospitalization increased for all age subgroups (<1, 1-5, 6-11, and 12-17 years), with the largest increase noted among children <1 year of age (from 18.1 per 100000 during 1994 to 49.6 per 100000 during 2009). Compared with 1994-1997, the adjusted odds of hospitalization with a VTE diagnosis were 88% higher during 2006-2009 (adjusted odds ratio: 1.88 [95% confidence interval: 1.64-2.17]). Venous catheter use, mechanical ventilation, malignancy, hospitalization ≥ 5 days, and VTE-related medical conditions were associated with increased likelihood of VTE diagnosis.
The rate of VTE-associated hospitalization among US children increased from 1994 through 2009. Increases in venous catheter procedures were associated with and may have contributed to the observed trends. The degree to which increased awareness of VTE influenced the temporal differences could not be determined.
美国儿童静脉血栓栓塞症(VTE)的相关信息稀缺且不一致。本研究旨在评估美国儿科 VTE 住院的相关趋势。
纳入了 1994 年至 2009 年全美住院患者样本中年龄在 0 至 17 岁之间的所有非常规新生儿住院患者;排除了常规新生儿出院患者。通过使用国际疾病分类,第 9 版临床修正版(ICD-9-CM)代码来确定 VTE 诊断。采用方差加权最小二乘法回归来评估各年龄段患者特征和每 10 万<18 岁人群住院率的趋势。多变量逻辑回归模型用于估计研究期间 VTE 诊断的概率。
所有年龄组(<1 岁、1-5 岁、6-11 岁和 12-17 岁)的 VTE 相关住院率均增加,<1 岁年龄组的增幅最大(从 1994 年的每 10 万人 18.1 例增加到 2009 年的每 10 万人 49.6 例)。与 1994 年至 1997 年相比,2006 年至 2009 年 VTE 诊断的调整后住院几率增加了 88%(调整后比值比:1.88[95%置信区间:1.64-2.17])。静脉置管、机械通气、恶性肿瘤、住院≥5 天和与 VTE 相关的医疗状况与 VTE 诊断的可能性增加相关。
美国儿童 VTE 相关住院率从 1994 年到 2009 年增加。静脉置管程序的增加与观察到的趋势相关,并且可能促成了这种趋势。无法确定增加对 VTE 的认识在多大程度上影响了时间差异。