Department of Epidemiology, Division of Biology and Medicine, Brown University, Providence, Rhode Island, USA.
Cancer Res. 2012 Oct 1;72(19):5004-13. doi: 10.1158/0008-5472.CAN-11-3277. Epub 2012 Sep 18.
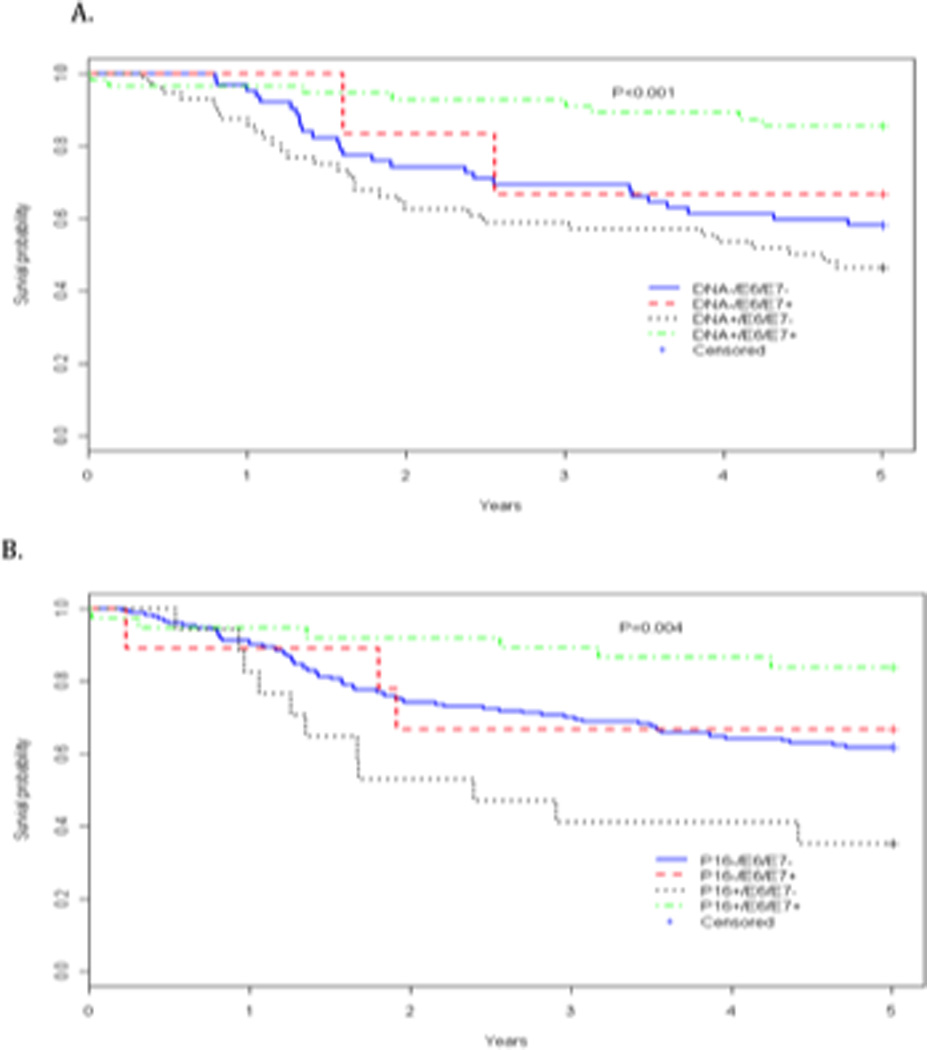
Human papillomavirus (HPV) is an accepted cause of head and neck squamous cell carcinoma (HNSCC), and patients with HPV-associated HNSCC have a favorable prognosis. Currently, there is no general guidance on the most appropriate biomarkers for clinical assessment of HPV in these malignancies. We compared PCR-based and serologic HPV assays, as well as p16 immunohistochemistry, individually and in combination in a single population-based study to assess their associations with overall survival among patients with HNSCC, and thus their potential value as biomarkers. HPV16 serology was determined for 488 patients; immunohistochemical detection of p16 expression in tumors was conducted in a subset of 233 cases, and PCR-based methods to assess the presence of HPV16 DNA in a subset of 179 cases of tumors. Considering each biomarker individually in the subset of patients studied for all endpoints, seropositivity for the E6 and E7 proteins was significantly associated with enhanced all-cause survival in oropharyngeal disease [HR(E6/E7+) = 0.1, 95% confidence interval (CI) = 0.02-0.3]. Neither the presence of HPV16 DNA nor p16 immunostaining was associated with significant enhanced overall survival in oropharyngeal disease (HR(DNA) = 0.9, 95% CI = 0.3-2.9; HR(p16) = 0.3, 95% CI = 0.1-1.1). However, the combination of HPV-positive DNA and E6 or E7 serology was associated with enhanced overall survival in oropharyngeal disease (HR(DNA+/E6/E7+) = 0.1, 95% CI = 0.02-1.0), whereas E6/E7 seronegative patients with evidence of HPV in tumor DNA did not show any evidence of favorable survival (HR(DNA+/E6-/E7-) = 3.4, 95% CI = 0.6-18.1). Furthermore, patients with p16 staining and E6 or E7 seropositivity had favorable survival from oropharyngeal disease (HR(p16+/E6/E7+) = 0.1, 95% CI = 0.02-0.4), whereas patients who were p16 positive and E6/E7 seronegative had significantly increased hazard of all causes of death (HR(p16+/E6-/E7-) = 3.1, 95% CI = 1.2-7.7). A stronger association of HPV presence with prognosis (assessed by all-cause survival) is observed when "HPV-associated" HNSCC is defined using tumor status (HPV DNA status or P16) and HPV E6/E7 serology in combination rather using tumor HPV status alone.
人乳头瘤病毒(HPV)是头颈部鳞状细胞癌(HNSCC)的公认病因,HPV 相关 HNSCC 患者的预后较好。目前,对于这些恶性肿瘤中 HPV 临床评估最合适的生物标志物,尚无一般指导。我们比较了基于聚合酶链反应(PCR)和血清学 HPV 检测以及肿瘤 p16 免疫组化在单一人群研究中的个体和联合应用,以评估它们与 HNSCC 患者总生存的相关性,从而评估它们作为生物标志物的潜在价值。对 488 例患者进行了 HPV16 血清学检测;在 233 例患者的肿瘤中进行了 p16 表达的免疫组化检测,在 179 例肿瘤的肿瘤中进行了基于 PCR 的 HPV16 DNA 检测。在研究所有终点的患者亚组中单独考虑每个生物标志物,E6 和 E7 蛋白的血清阳性与口咽疾病的全因生存改善显著相关[HR(E6/E7+)=0.1,95%置信区间(CI)=0.02-0.3]。HPV16 DNA 或 p16 免疫染色均与口咽疾病的总生存无显著相关性增强(HR(DNA)=0.9,95%CI=0.3-2.9;HR(p16)=0.3,95%CI=0.1-1.1)。然而,HPV 阳性 DNA 和 E6 或 E7 血清学的联合与口咽疾病的总生存改善相关(HR(DNA+/E6/E7+)=0.1,95%CI=0.02-1.0),而肿瘤 DNA 中 HPV 呈阳性且 E6/E7 血清学阴性的患者无任何生存获益证据(HR(DNA+/E6-/E7-)=3.4,95%CI=0.6-18.1)。此外,p16 染色和 E6 或 E7 血清学阳性的患者口咽疾病的生存情况较好(HR(p16+/E6/E7+)=0.1,95%CI=0.02-0.4),而 p16 阳性且 E6/E7 血清学阴性的患者全因死亡的风险显著增加(HR(p16+/E6-/E7-)=3.1,95%CI=1.2-7.7)。当使用肿瘤状态(HPV DNA 状态或 P16)和 HPV E6/E7 血清学联合而非单独使用肿瘤 HPV 状态来定义“HPV 相关”HNSCC 时,与预后(通过全因生存评估)的 HPV 存在的相关性更强。