Section of Orthopedics and Sports Medicine, Department of Molecular Medicine and Surgery, Stockholm Sports Trauma Research Center, Karolinska Institutet, Stockholm, Sweden.
Sports Health. 2012 May;4(3):193-201. doi: 10.1177/1941738112440957.
Tendinopathy is increasing in prevalence and accounts for a substantial part of all sports injuries and occupational disorders. Despite the magnitude of the disorder, high-quality scientific data on etiology and available treatments have been limited.
The authors conducted a MEDLINE search on tendinopathy, or "tendonitis" or "tendinosis" or "epicondylitis" or "jumpers knee" from 1980 to 2011. The emphasis was placed on updates on epidemiology, etiology, and recent patient-oriented Level 1 literature.
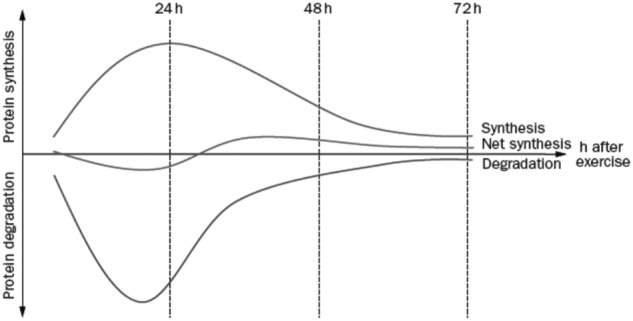
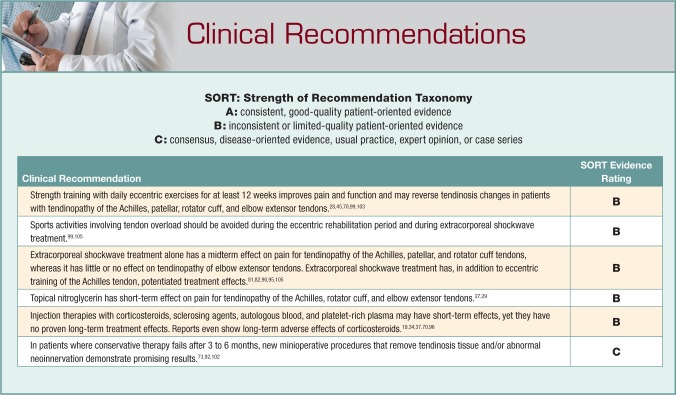
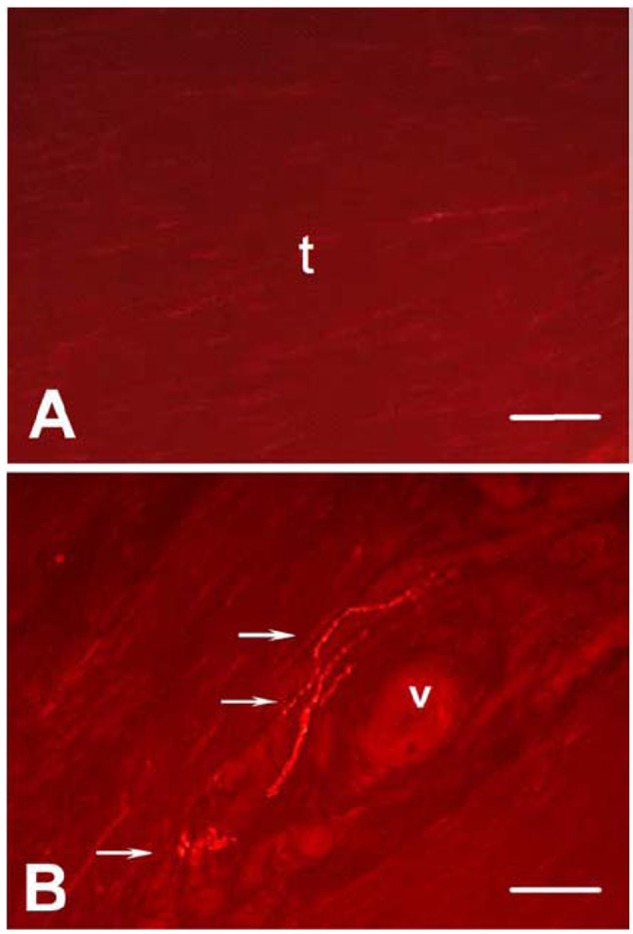
Repetitive exposure in combination with recently discovered intrinsic factors, such as genetic variants of matrix proteins, and metabolic disorders is a risk factor for the development of tendinopathy. Recent findings demonstrate that tendinosis is characterized by a fibrotic, failed healing response associated with pathological vessel and sensory nerve ingrowth. This aberrant sensory nerve sprouting may partly explain increased pain signaling and partly, by release of neuronal mediators, contribute to the fibrotic alterations observed in tendinopathy. The initial nonoperative treatment should involve eccentric exercise, which should be the cornerstone (basis) of treatment of tendinopathy. Eccentric training combined with extracorporeal shockwave treatment has in some reports shown higher success rates compared to any therapies alone. Injection therapies (cortisone, sclerosing agents, blood products including platelet-rich plasma) may have short-term effects but have no proven long-term treatment effects or meta-analyses to support them. For epicondylitis, cortisone injections have demonstrated poorer long-time results than conservative physiotherapy. Today surgery is less indicated because of successful conservative therapies. New minioperative procedures that, via the endoscope, remove pathologic tissue or abnormal neoinnervation demonstrate promising results but need confirmation by Level 1 studies.
Novel targeted therapies are emerging, but multicenter trials are needed to confirm the results of exercise and mini-invasive treatments.
肌腱病的发病率不断上升,在所有运动损伤和职业疾病中占很大比例。尽管这种疾病的程度很严重,但关于病因和现有治疗方法的高质量科学数据一直很有限。
作者对肌腱病(或“腱炎”或“腱病”或“肱骨外上髁炎”或“跳跃膝”)进行了 MEDLINE 搜索,时间范围为 1980 年至 2011 年。重点是更新流行病学、病因学和最近面向患者的一级文献。
反复暴露加上最近发现的内在因素,如基质蛋白的遗传变异和代谢紊乱,是肌腱病发展的一个危险因素。最近的研究结果表明,腱病的特征是纤维化、愈合失败反应,与病理性血管和感觉神经生长有关。这种异常感觉神经的萌芽可能部分解释了疼痛信号的增加,并通过神经元介质的释放,部分导致了肌腱病中观察到的纤维化改变。最初的非手术治疗应包括离心运动,这应是治疗肌腱病的基石。离心训练结合体外冲击波治疗在一些报告中显示出比任何单一治疗更高的成功率。注射治疗(皮质类固醇、硬化剂、包括富含血小板的血浆在内的血液制品)可能有短期效果,但没有长期治疗效果的证据或荟萃分析支持。对于肱骨外上髁炎,皮质类固醇注射的长期效果比保守物理治疗差。如今,由于成功的保守治疗,手术的指征较少。新的微创手术程序,通过内窥镜切除病理性组织或异常的新生神经支配,显示出有前途的结果,但需要一级研究的证实。
新的靶向治疗方法正在出现,但需要多中心试验来证实运动和微创治疗的结果。