Escola Nacional de Saúde Pública, Universidade Nova de Lisboa, Lisboa, Lisboa, Portugal.
PLoS One. 2012;7(9):e44774. doi: 10.1371/journal.pone.0044774. Epub 2012 Sep 17.
Current Portuguese HIV treatment guidelines recommend initiating antiretroviral therapy with a regimen composed of two Nucleoside Reverse Transcriptase Inhibitors plus one Non-nucleoside Reverse Transcriptase Inhibitor (2NRTI+NNRTI) or two Nucleoside Reverse Transcriptase Inhibitors plus one boosted protease inhibitor (2NRTI+PI/r). Given the lower daily cost of NNRTI as the third agent when compared to the average daily costs of PI/r, it is relevant to estimate the long term impact of each treatment option in the Portuguese context.
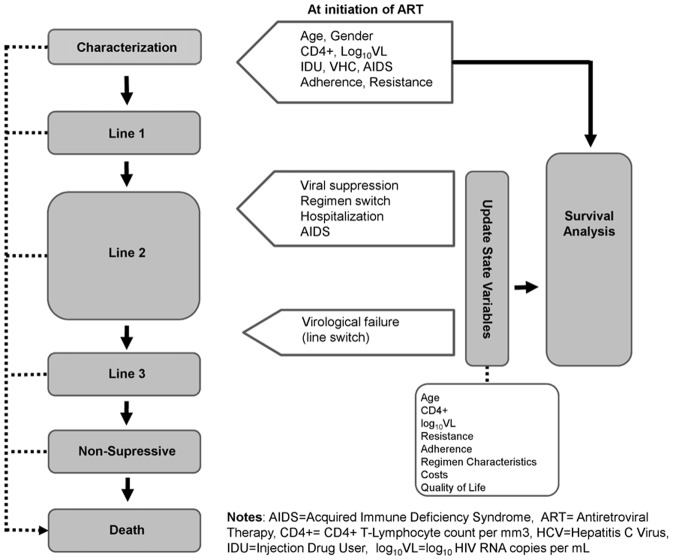
We developed a microsimulation discrete events model for cost-effectiveness analysis of HIV treatment, simulating individual paths from ART initiation to death. Four driving forces determine the course of events: CD4+ cell count, viral load, resistance and adherence. Distributions of time to event are conditional to individuals' characteristics and past history. Time to event was modeled using parametric survival analysis using Stata 11®. Disease progression was structured according to therapy lines and the model was parameterized with cohort Portuguese observational data. All resources were valued at 2009 prices. The National Health Service's perspective was assumed considering a lifetime horizon and a 5% annual discount rate.
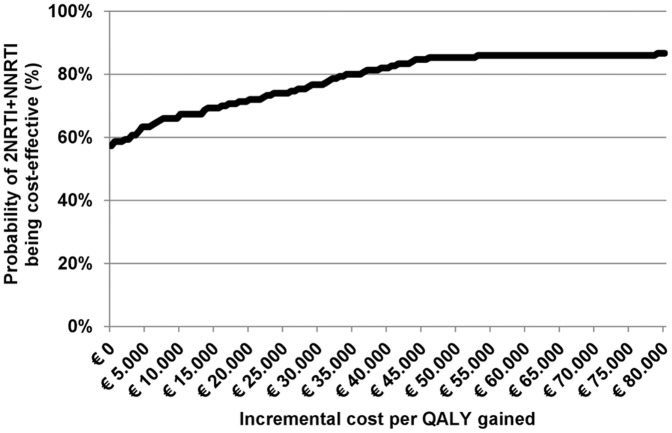
In this analysis, initiating therapy with two Nucleoside Reverse Transcriptase Inhibitors plus one Non-nucleoside Reverse Transcriptase Inhibitor reduces the average number of switches by 17%, saves 19.573€ per individual and increases life expectancy by 1.7 months showing to be a dominant strategy in 57% of the simulations when compared to two Nucleoside Reverse Transcriptase Inhibitors plus one boosted protease inhibitor.
This study suggests that, when clinically valid, initiating therapy with two Nucleoside Reverse Transcriptase Inhibitors plus one Non-nucleoside Reverse Transcriptase Inhibitor is a cost-saving strategy and equally effective when compared to two Nucleoside Reverse Transcriptase Inhibitors plus one boosted protease inhibitor as the first regimen.
目前,葡萄牙的艾滋病毒治疗指南建议采用由两种核苷类逆转录酶抑制剂加一种非核苷类逆转录酶抑制剂(2NRTI+NNRTI)或两种核苷类逆转录酶抑制剂加一种增效蛋白酶抑制剂(2NRTI+PI/r)组成的方案启动抗逆转录病毒治疗。鉴于与 PI/r 的平均日费用相比,NNRTI 作为第三种药物的每日费用较低,因此有必要根据葡萄牙的情况估计每种治疗方案的长期影响。
我们开发了一种用于艾滋病毒治疗成本效益分析的微观模拟离散事件模型,模拟从开始接受抗逆转录病毒治疗到死亡的个体路径。有四个驱动因素决定事件的进程:CD4+细胞计数、病毒载量、耐药性和依从性。事件时间的分布取决于个人的特征和过去的历史。使用 Stata 11®进行参数生存分析来建模事件时间。疾病进展根据治疗线进行构建,模型根据葡萄牙队列观察数据进行参数化。所有资源均按 2009 年的价格进行估值。假设从国家卫生服务的角度考虑,采用终身视野和 5%的年贴现率。
在这项分析中,与采用两种核苷类逆转录酶抑制剂加一种增效蛋白酶抑制剂相比,采用两种核苷类逆转录酶抑制剂加一种非核苷类逆转录酶抑制剂治疗可减少平均 17%的药物转换次数,为每位患者节省 19,573 欧元,并使预期寿命延长 1.7 个月,在 57%的模拟中,与采用两种核苷类逆转录酶抑制剂加一种增效蛋白酶抑制剂相比,这种策略具有优势。
本研究表明,在临床可行的情况下,与采用两种核苷类逆转录酶抑制剂加一种增效蛋白酶抑制剂相比,采用两种核苷类逆转录酶抑制剂加一种非核苷类逆转录酶抑制剂作为初始方案是一种节省成本的策略,与采用两种核苷类逆转录酶抑制剂加一种增效蛋白酶抑制剂的方案同样有效。