KEMRI,Wellcome Centre for Geographic Medicine and Research, Coast, PO BOX 230, Kilifi 80108, Kenya.
Early Hum Dev. 2012 Dec;88(12):957-60. doi: 10.1016/j.earlhumdev.2012.09.005. Epub 2012 Sep 30.
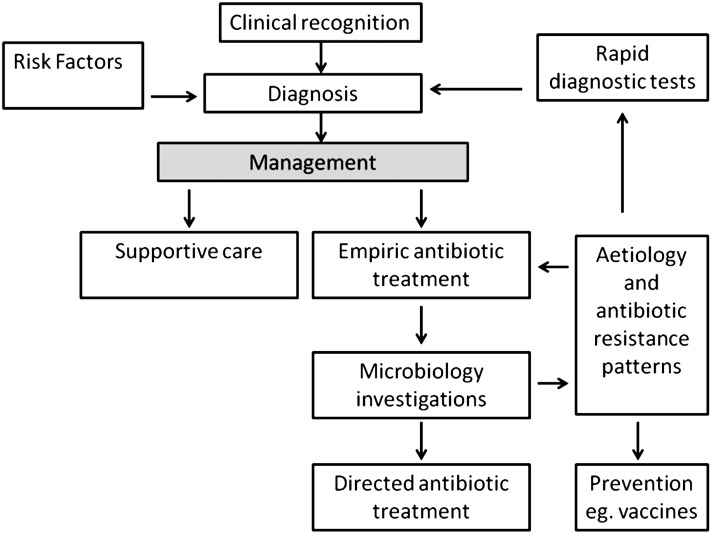
Reducing childhood mortality in resource-poor regions depends on effective interventions to decrease neonatal mortality from severe infection, which contributes up to a half of all neonatal deaths. There are key differences in resource-poor, compared to resource-rich, countries in terms of diagnosis, supportive care and treatment. In resource-poor settings, diagnosis is based on identifying clinical syndromes from international guidelines; microbiological investigations are restricted to a few research facilities. Low levels of staffing and equipment limit the provision of basic supportive care, and most facilities cannot provide respiratory support. Empiric antibiotic treatment guidelines are based on few aetiological and antimicrobial susceptibility data. Research on improving health care systems to provide effective supportive care, and implementation of simple pragmatic interventions, such as low-cost respiratory support, are essential, together with improved surveillance to monitor emerging drug resistance and treatment failures. Reductions in mortality will also be achieved through prevention of infection; including emerging vaccination and anti-sepsis strategies.
降低资源匮乏地区的儿童死亡率取决于有效干预措施,以降低严重感染导致的新生儿死亡率,严重感染导致的新生儿死亡约占所有新生儿死亡的一半。在资源匮乏国家和资源丰富国家,在诊断、支持性护理和治疗方面存在着关键的差异。在资源匮乏的环境中,诊断是基于从国际指南中识别临床综合征;微生物学调查仅限于少数研究机构。人员配备和设备水平低,限制了基本支持性护理的提供,而且大多数设施无法提供呼吸支持。经验性抗生素治疗指南是基于为数不多的病因和抗菌药物敏感性数据制定的。改善医疗保健系统以提供有效支持性护理的研究,以及实施简单实用的干预措施,如低成本呼吸支持,是至关重要的,同时还需要加强监测,以监测新出现的耐药性和治疗失败情况。通过预防感染,包括新出现的疫苗接种和抗脓毒症策略,也可以降低死亡率。