Division of Endocrinology, Hospital de Clínicas de Porto Alegre, Porto Alegre, Brazil.
Lipids Health Dis. 2012 Oct 9;11:133. doi: 10.1186/1476-511X-11-133.
Much attention has been drawn to the deleterious effects of adding progestins to estrogen as hormone therapy (HT) in postmenopausal women. Some widely prescribed progestins have been shown to partially oppose the beneficial effects of estrogens on surrogate markers of cardiovascular disease (CVD) risk. Progestins with higher androgenic activity may interfere with lipid profile and glucose tolerance, and could affect mechanisms of estrogen-induced C-reactive protein (CRP) stimulation. Recent data have shown that norpregnane derivatives, but not micronized progesterone, increase the risk of venous thromboembolism among transdermal estrogens users. The aim of the present study was to assess the effects of combining micronized progesterone with non-oral estrogen therapy on lipid profile and cardiovascular risk factors in a sample of early postmenopausal women.
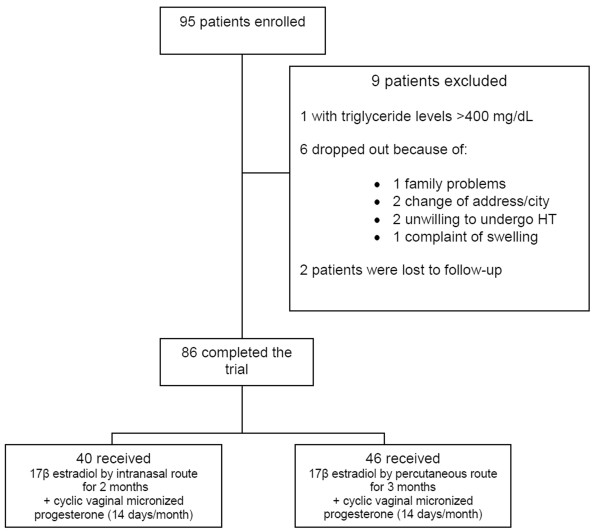
Clinical trial including 40 women receiving intranasal 17β estradiol 3 mg/day for two months and 46 women receiving percutaneous 17β estradiol gel 1.5 mg/day for three months (E2). Both groups received an additional 200 mg/day of micronized progesterone by vaginal route 14 days/month (E2+P). Outcome measures included body weight, waist circumference, body mass index (BMI), lipid profile and ultra-sensitive C-reactive protein (usCRP) at baseline and during the E2 or E2+P portions of treatment.
Mean age was 51±3 years. Mean time since menopause was 22.2±10 months. Most participants were overweight; HT did not change BMI. E2 and E2+P did not affect waist circumference and weight. Menopausal symptoms improved after HT. The effects of intranasal and percutaneous estradiol were similar, regardless of the addition of progesterone. Similarly, for the overall group of 86 women, micronized progesterone did not alter the response to E2. Blood pressure, glucose, insulin, HDL-c, triglycerides, and usCRP remained constant with or without micronized progesterone. Total cholesterol decreased after E2, and progesterone maintained this reduction. LDL-c levels were similar at baseline and with E2, and lower during E2+P in relation to baseline.
Cyclic, short term exposure to vaginal micronized progesterone did not alter the metabolic and cardiovascular effects of non-oral E2 in early, apparently healthy, postmenopausal women.
ClinicalTrials.gov NCT01432028.
在绝经后妇女中,将孕激素添加到雌激素作为激素替代疗法(HT)已引起人们的关注。一些广泛使用的孕激素已被证明部分抵消了雌激素对心血管疾病(CVD)风险替代标志物的有益作用。雄激素活性较高的孕激素可能会干扰血脂谱和葡萄糖耐量,并可能影响雌激素诱导的 C 反应蛋白(CRP)刺激的机制。最近的数据表明,诺孕烷衍生物而不是微粒化黄体酮,会增加经皮雌激素使用者发生静脉血栓栓塞的风险。本研究的目的是评估米诺孕醇与非口服雌激素联合治疗对早期绝经后妇女血脂谱和心血管危险因素的影响。
临床试验纳入了 40 名接受鼻腔内 17β 雌二醇 3mg/天治疗两个月的女性和 46 名接受经皮 17β 雌二醇凝胶 1.5mg/天治疗三个月的女性(E2)。两组均在阴道途径上接受 200mg/天的米诺孕醇,每月 14 天(E2+P)。在基线和 E2 或 E2+P 治疗期间,评估了体重、腰围、体重指数(BMI)、血脂谱和超敏 C 反应蛋白(usCRP)。
平均年龄为 51±3 岁。绝经后平均时间为 22.2±10 个月。大多数参与者超重;HT 未改变 BMI。E2 和 E2+P 不影响腰围和体重。绝经后症状在 HT 后得到改善。鼻内和经皮雌激素的作用相似,与孕激素的添加无关。同样,对于 86 名女性的总体人群,米诺孕醇并未改变对 E2 的反应。血压、血糖、胰岛素、HDL-c、甘油三酯和 usCRP 在有无米诺孕醇的情况下保持不变。E2 后总胆固醇降低,孕激素维持此降低。LDL-c 水平在基线和 E2 时相似,E2+P 时与基线相比降低。
短期、周期性阴道使用米诺孕醇不会改变非口服 E2 在早期、明显健康的绝经后妇女中的代谢和心血管作用。
ClinicalTrials.gov NCT01432028。