Amgen (Europe) GmbH, Dammstrasse 23, 6300, Zug, Switzerland.
BMC Nephrol. 2012 Oct 29;13:140. doi: 10.1186/1471-2369-13-140.
Secondary hyperparathyroidism (SHPT) is associated with mortality in patients with chronic kidney disease (CKD), but the economic consequences of SHPT have not been adequately studied in the European population. We assessed the relationship between SHPT parameters (intact parathyroid hormone [iPTH], calcium, and phosphate) and hospitalisations, medication use, and associated costs among CKD patients in Europe.
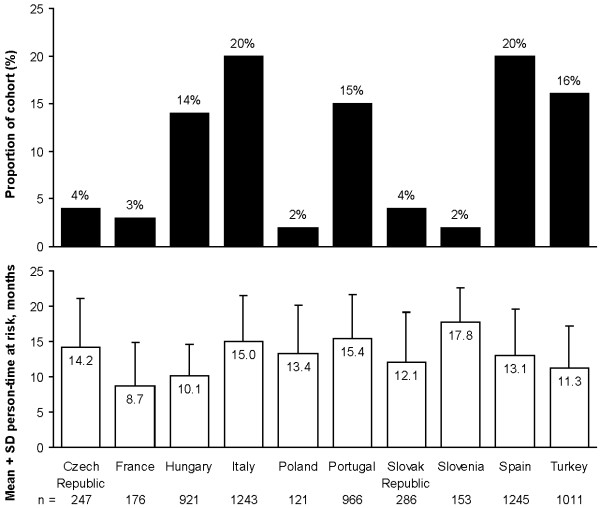
The analysis of this retrospective cohort study used records of randomly selected patients who underwent haemodialysis between January 1, 2005 and December 31, 2006 at participating European Fresenius Medical Care facilities in 10 countries. Patients had ≥ 1 iPTH value recorded, and ≥ 1 month of follow-up after a 3-month baseline period during which SHPT parameters were assessed. Time at risk was post-baseline until death, successful renal transplantation, loss to follow-up, or the end of follow-up. Outcomes included cost per patient-month, rates of hospitalisations (cardiovascular disease [CVD], fractures, and parathyroidectomy [PTX]), and use of SHPT-, diabetes-, and CVD-related medications. National costs were applied to hospitalisations and medication use. Generalised linear models compared costs across strata of iPTH, total calcium, and phosphate, adjusting for baseline covariates.
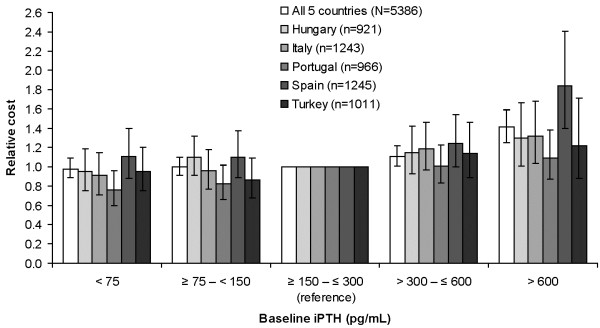
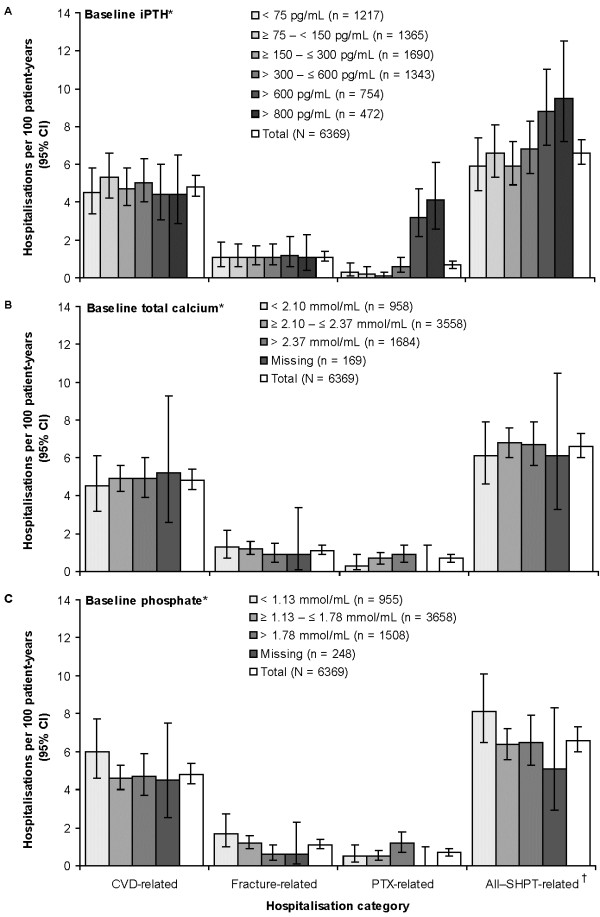
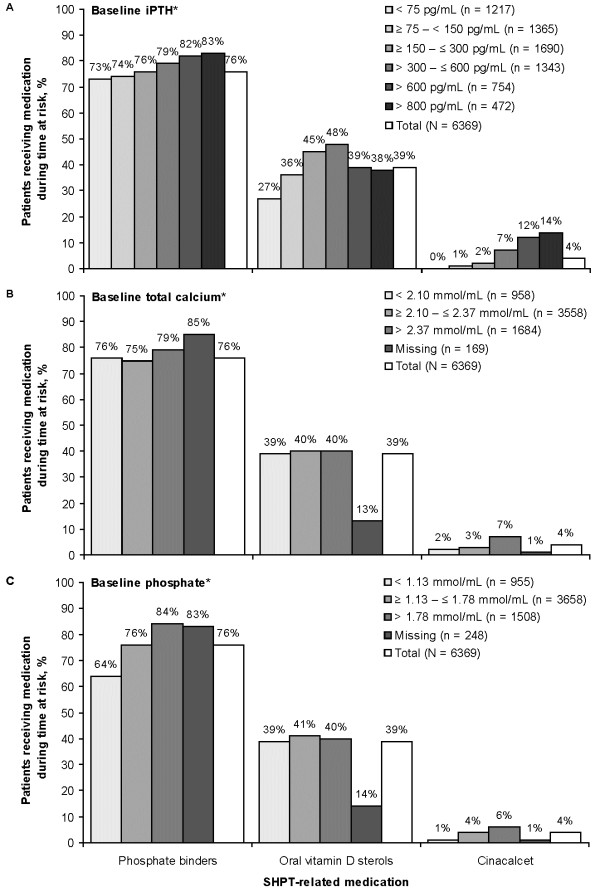
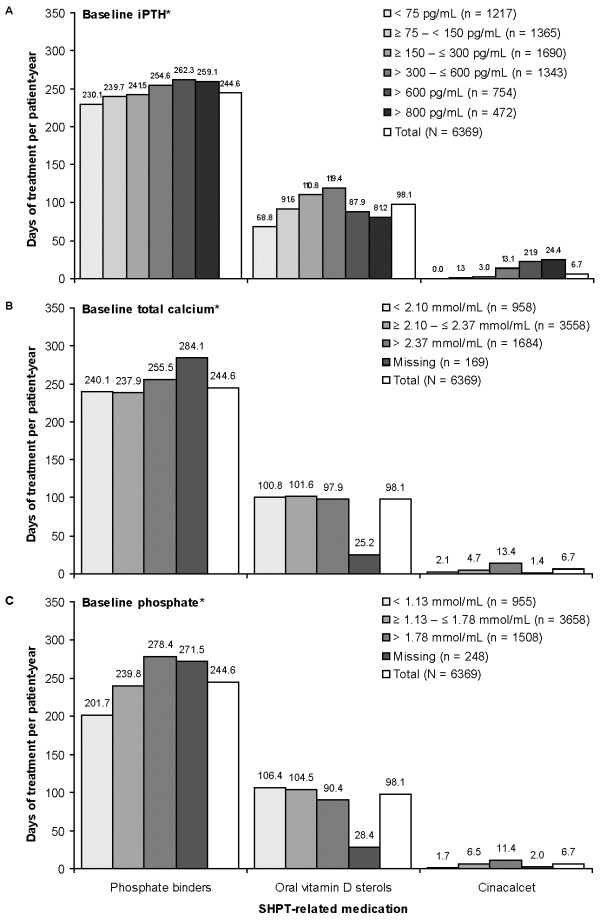
There were 6369 patients included in the analysis. Mean ± SD person-time at risk was 13.1 ± 6.4 months. Patients with iPTH > 600 pg/mL had a higher hospitalisation rate than those with lower iPTH. Hospitalisation rates varied little across calcium and phosphate levels. SHPT-related medication use varied with iPTH, calcium, and phosphate. After adjusting for demographic and clinical variables, patients with baseline iPTH > 600 pg/mL had 41% (95% CI: 25%, 59%) higher monthly total healthcare costs compared with those with iPTH in the K/DOQI target range (150-300 pg/mL). Patients with baseline phosphate and total calcium levels above target ranges (1.13-1.78 mmol/L and 2.10-2.37 mmol/L, respectively) had 38% (95% CI: 27%, 50%) and 8% (95% CI: 0%, 17%) higher adjusted monthly costs, respectively. Adjusted costs were 25% (95% CI: 18%, 32%) lower among patients with baseline phosphate levels below the target range. Results were consistent in sensitivity analyses.
These data suggest that elevated SHPT parameters increase the economic burden of CKD in Europe.
继发性甲状旁腺功能亢进症(SHPT)与慢性肾脏病(CKD)患者的死亡率相关,但在欧洲人群中,SHPT 的经济后果尚未得到充分研究。我们评估了欧洲 CKD 患者的 SHPT 参数(全段甲状旁腺激素[iPTH]、钙和磷)与住院、药物使用和相关费用之间的关系。
本回顾性队列研究分析使用了 2005 年 1 月 1 日至 2006 年 12 月 31 日期间在欧洲 Fresenius 医疗保健设施接受血液透析的随机选择患者的记录。患者有≥1 次 iPTH 值记录,并且在 3 个月的基线期后至少有 1 个月的随访,在此期间评估了 SHPT 参数。风险时间为基线后至死亡、成功肾移植、失访或随访结束。结局包括每位患者每月的费用、住院率(心血管疾病 [CVD]、骨折和甲状旁腺切除术 [PTX])以及 SHPT、糖尿病和 CVD 相关药物的使用。将国家费用应用于住院和药物使用。广义线性模型比较了不同 iPTH、总钙和磷水平分层的成本,调整了基线协变量。
分析纳入了 6369 名患者。风险期间的平均±SD 人时为 13.1±6.4 个月。iPTH>600 pg/mL 的患者的住院率高于 iPTH 较低的患者。在钙和磷水平上,住院率变化不大。SHPT 相关药物的使用随 iPTH、钙和磷而变化。在调整了人口统计学和临床变量后,基线 iPTH>600 pg/mL 的患者与 K/DOQI 目标范围内(150-300 pg/mL)的患者相比,每月总医疗保健费用增加了 41%(95%CI:25%,59%)。基线时磷和总钙水平高于目标范围(分别为 1.13-1.78 mmol/L 和 2.10-2.37 mmol/L)的患者,调整后的每月费用分别增加了 38%(95%CI:27%,50%)和 8%(95%CI:0%,17%)。基线时磷水平低于目标范围的患者,调整后的成本降低了 25%(95%CI:18%,32%)。敏感性分析结果一致。
这些数据表明,升高的 SHPT 参数增加了欧洲 CKD 的经济负担。