Department of Pharmacy Clinical Outcomes and Economics Group, Renji Hospital, affiliated with the School of Medicine, Shanghai Jiaotong University, Dongfang Road 1630, Shanghai, China.
BMC Health Serv Res. 2012 Nov 8;12:385. doi: 10.1186/1472-6963-12-385.
Several rescue therapies have been used in patients with lamivudine (LAM)-resistant chronic hepatitis B (CHB); however, the economic outcome of these therapies is unclear. The object of the current analysis was to evaluate the lifetime cost-effectiveness of rescue therapies among patients with LAM-resistant CHB.
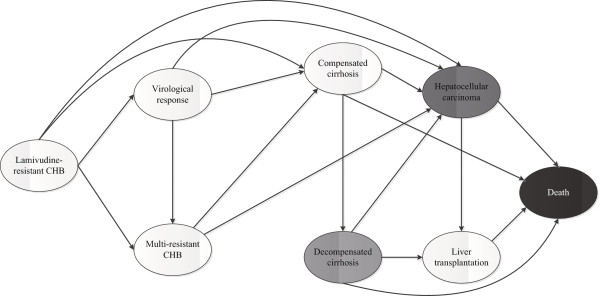
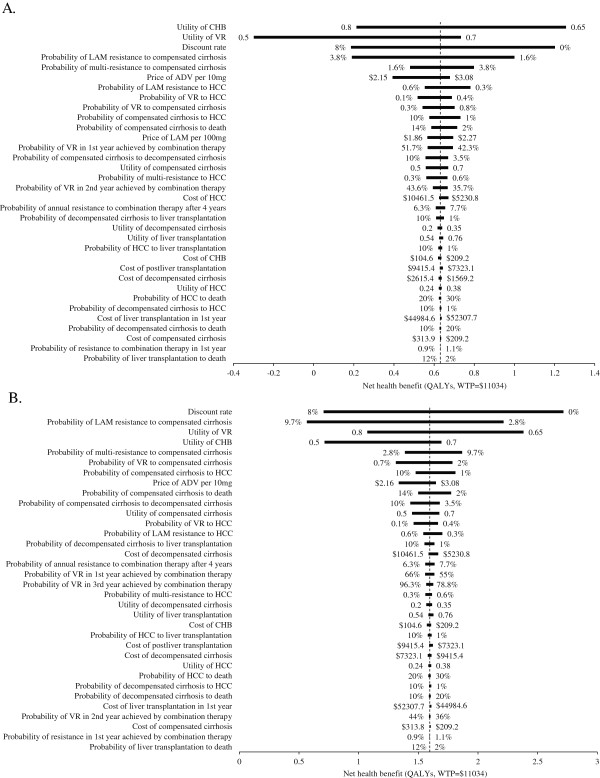
A Markov model was developed to simulate the clinical course of patients with LAM-resistant CHB. From the perspective of Chinese health care, a lifetime cost-utility analysis was performedfor 4 rescue strategies: adefovir (ADV), entecavir (ETV) or tenofovir (TDF) monotherapy and combination therapy using LAM and ADV. A hypothetical cohort of 45-year-old patients with genotypic or clinical LAM-resistant CHB entered the model, and the beginning health state was LAM-resistant CHB without other complications. The transition probabilities, efficacy and resistance data for each rescue therapy as well as the costs and utility data were estimated from the literature. The discount rate (3%) utilized for costs and benefits. Sensitivity analyses were used to explore the impact of uncertainty on the results.
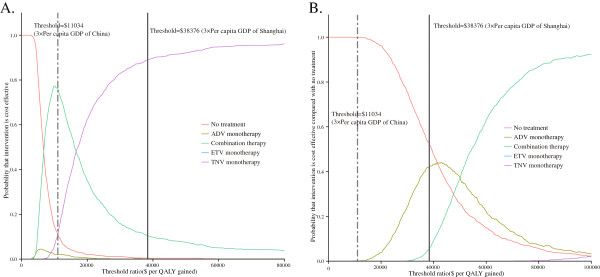
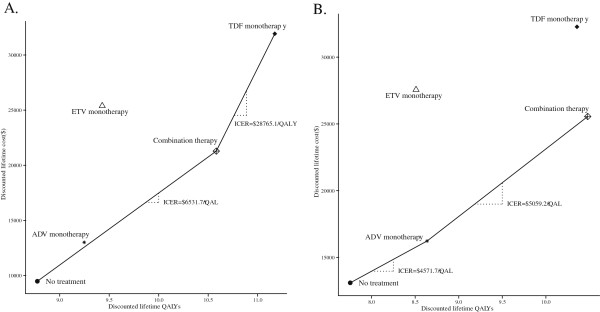
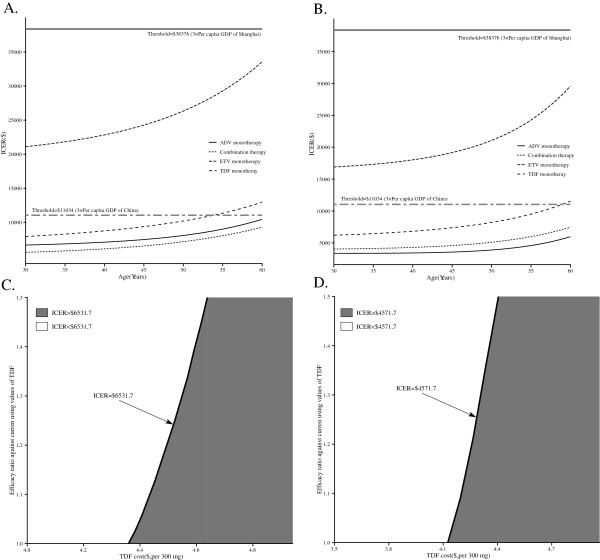
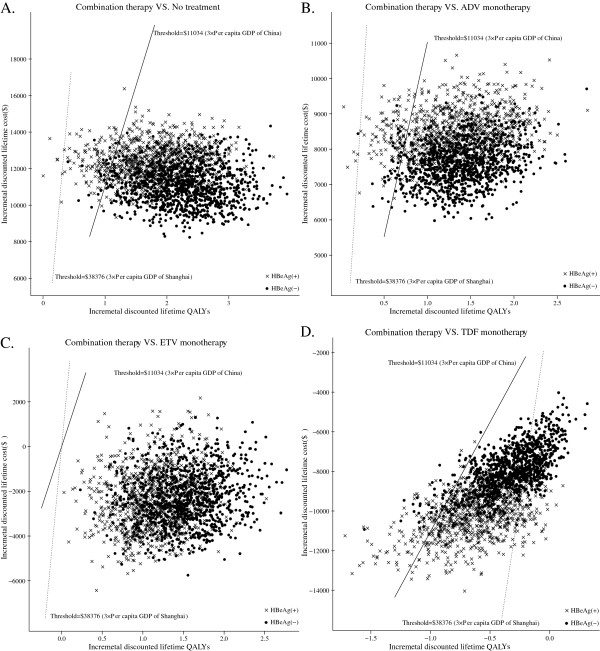
In LAM-resistant HBeAg-positive and HBeAg-negative CHB cohorts, TDF monotherapy and combination therapy were on the efficiency frontier for both positive and negative populations. Compared with no treatment, the use of combination therapy cost an additional $6,531.7 to gain 1 additional quality-adjusted life year (QALY) for HBeAg-positive patients and $4,571.7 to gain 1 additional QALY for HBeAg-negative patients. TDF monotherapy for HBeAg-positive patients, shows greater increase in QALYs but higher incremental cost-effectiveness ratio (ICER) in comparison with combination therapy. In probabilistic sensitivity analyses, combination therapy was the preferred option for health care systems with limited health resources, such as Chinese health care system.
In Chinese patients with LAM-resistant CHB, combination therapy is a more cost-effective option than the competing rescue therapies.
已有多种挽救疗法用于治疗拉米夫定(LAM)耐药的慢性乙型肝炎(CHB)患者,但这些疗法的经济学结局尚不清楚。本分析旨在评估 LAM 耐药 CHB 患者接受挽救治疗的终生成本效益。
采用 Markov 模型模拟 LAM 耐药 CHB 患者的临床病程。从中国卫生保健的角度出发,对 4 种挽救治疗策略(阿德福韦酯[ADV]、恩替卡韦[ETV]或替诺福韦[TDF]单药治疗以及 LAM 联合 ADV 的联合治疗)进行了终生成本-效用分析。假设 45 岁的基因型或临床 LAM 耐药 CHB 患者进入模型,起始健康状态为无其他并发症的 LAM 耐药 CHB。每种挽救治疗的转归概率、疗效和耐药数据以及成本和效用数据均来自文献。采用 3%的贴现率(年)对成本和获益进行贴现。敏感性分析用于探究不确定性对结果的影响。
在 LAM 耐药 HBeAg 阳性和 HBeAg 阴性 CHB 队列中,TDF 单药治疗和联合治疗在阳性和阴性人群中均处于效率前沿。与未治疗相比,HBeAg 阳性患者采用联合治疗每获得 1 个额外质量调整生命年(QALY)需多花费 6531.7 美元,HBeAg 阴性患者每获得 1 个额外 QALY 需多花费 4571.7 美元。与联合治疗相比,TDF 单药治疗可使 HBeAg 阳性患者获得更多的 QALY,但增量成本-效用比(ICER)更高。在概率敏感性分析中,对于中国卫生保健系统等资源有限的卫生保健系统而言,联合治疗是更具成本效益的选择。
在中国 LAM 耐药 CHB 患者中,与其他挽救治疗相比,联合治疗是更具成本效益的选择。