Department of Rheumatology, Queen Elizabeth Hospital Birmingham, Birmingham, UK.
BMJ Open. 2012 Nov 12;2(6). doi: 10.1136/bmjopen-2012-001395. Print 2012.
To compare adalimumab versus etanercept in patients with active rheumatoid arthritis (RA) to test the hypothesis that adalimumab was not inferior to etanercept in terms of drug continuation by a margin of 15% after 52 weeks of treatment.
Pragmatic, randomised, parallel group, multicentre, unblinded and non-inferiority trial. Randomisation stratified by baseline use of methotrexate.
125 adults with active RA despite treatment with two disease-modifying drugs (DMARDs), including methotrexate randomised (1 : 1) to adalimumab 40 mg alternate weeks or etanercept 50 mg weekly, added to existing medication.
The primary outcome was proportion of patients continuing treatment after 52 weeks. Secondary outcomes included: disease activity score using 28 joints (DAS28), treatment satisfaction (TSQM V.2), health status (Euroqol-5D), drug toxicity and persistence with therapy after 2 years.
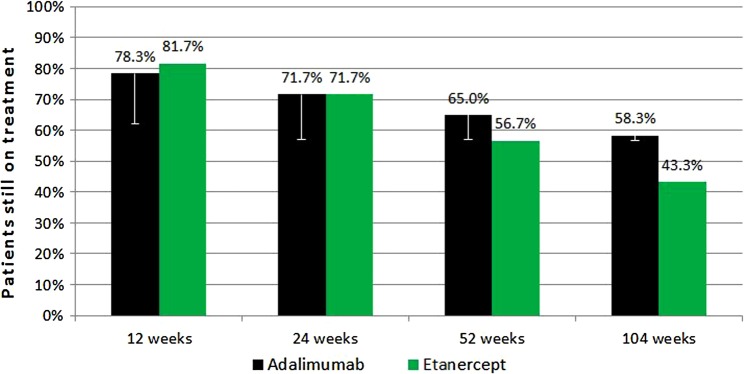
Persistence with therapy was 65% for adalimumab versus 56.7% for etanercept (one-sided 95% CI for proportion still taking adalimumab minus proportion on etanercept ≥-7.9%); demonstrating non-inferiority at the 15% margin. After 2 years these figures were: adalimumab 58.3% and etanecept 43.3% (CI ≥-1.7%). The proportion of good, moderate and non-responders based on DAS28-C reactive protein, after 52 weeks, were 26.3%, 33.3% and 40.4%, respectively, for adalimumab versus 16.7%, 31.7% and 51.7%, respectively, for etanercept (p=0.158). Baseline median EQ-5D scores improved from 0.52 to 0.69 for adalimumab and from 0.52 to 0.64 for etanercept (p=0.046) after 52 weeks. Global satisfaction, effectiveness, side effects and convenience scores based on the TSQM were similar for both drugs. Fourteen serious adverse events occurred including two deaths from myocardial infarction, one patient with ovarian cancer and one with acute myeloid leukaemia.
Clinicians choosing a first tumour necrosis factor inhibitor for active RA, despite trying two DMARDs including methotrexate, may choose either adalimumab or etanercept in the knowledge that these drugs are similarly effective.
EU Clinical Trials Register 2006-006275-21/GB.
比较阿达木单抗与依那西普在活动期类风湿关节炎(RA)患者中的疗效,以检验阿达木单抗在经过 52 周治疗后药物持续使用比例不低于依那西普 15%的假设。
实用、随机、平行分组、多中心、非盲、非劣效性试验。根据基线时是否使用甲氨蝶呤进行分层随机分组。
125 名活动性 RA 患者,尽管已接受两种疾病修饰药物(DMARDs)治疗,包括甲氨蝶呤,随机(1:1)分配至阿达木单抗 40mg 隔周或依那西普 50mg 每周治疗,同时加用现有药物。
主要结局为 52 周时继续治疗的患者比例。次要结局包括:使用 28 个关节疾病活动评分(DAS28)、治疗满意度(TSQM V.2)、健康状况(EuroQol-5D)、药物毒性和 2 年后治疗的持续情况。
阿达木单抗组的治疗持续率为 65%,依那西普组为 56.7%(单侧 95%CI 阿达木单抗组仍接受治疗的比例减去依那西普组的比例≥-7.9%);在 15%的差值上证明了非劣效性。2 年后,这些数据分别为阿达木单抗组 58.3%和依那西普组 43.3%(CI ≥-1.7%)。52 周后,根据 DAS28-C 反应蛋白,阿达木单抗组的良好、中等和无应答比例分别为 26.3%、33.3%和 40.4%,依那西普组分别为 16.7%、31.7%和 51.7%(p=0.158)。阿达木单抗组和依那西普组基线时的中位数 EQ-5D 评分分别从 0.52 提高至 0.69 和 0.52 提高至 0.64(p=0.046)。基于 TSQM 的全球满意度、有效性、副作用和便利性评分在两种药物之间相似。共发生 14 例严重不良事件,包括 2 例心肌梗死死亡、1 例卵巢癌和 1 例急性髓系白血病。
对于活动性 RA 患者,在尝试两种 DMARDs(包括甲氨蝶呤)后选择首种肿瘤坏死因子抑制剂的临床医生,可选择阿达木单抗或依那西普,因为这两种药物的疗效相似。
欧盟临床试验注册 2006-006275-21/GB。