Al Muradi Hazem, Mehra Aditya, Okolo Joseph, Vlachos Helen, Selzer Faith, Marroquin Oscar C, Skelding Kimberly, Holper Elizabeth M, Williams David O, Abbott J Dawn
Division of Cardiology, Rhode Island Hospital, Brown University, 593 Eddy St, Providence, RI 02903, USA.
Cardiovasc Revasc Med. 2012 Nov-Dec;13(6):311-5. doi: 10.1016/j.carrev.2012.10.003.
Drug eluting stent (DES) failure including restenosis and stent thrombosis, or disease progression may result in target vessel revascularization (TVR) but the relative contribution of these mechanisms in the DES era is not well described. We sought to examine the predictors and presentations of patients with clinically driven TVR after DES.
Patients with all lesions treated with a DES in the Dynamic Registry from 2004 to 2006 were analyzed. Included were 2691 patients with 3401 lesions. Patients with and without incident clinically driven TVR at 2years were compared according to baseline clinical, procedural, and angiographic characteristics and independent predictors of TVR and target lesion revascularization (TLR) were determined by multivariate analysis.
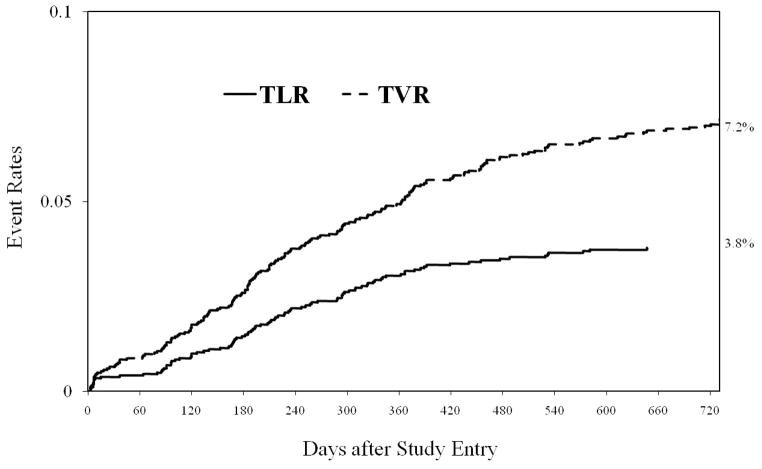
By 2-years, TVR occurred in 7.2% of patients and TLR in 3.8%, with 71.6% and 82.5% of repeat revascularization events occurring in the first year, respectively. The indication for first TVR was myocardial infarction in 18.6% (n=34), unstable angina in 42.6% (n=78), stable coronary disease in 25.7% (n=47) and other/unknown in 13.1% (n=24). Disease progression was responsible for 47% of TVR. Among patients with TLR, restenosis was the mechanism in 86.6% and stent thrombosis in 13.4%. Independent predictors of TVR included younger age, diabetes, attempted graft lesion, lesion length >30mm and prior lesion intervention. Independent predictors of TVR and TLR were similar.
The incidence of clinically driven TVR is low in patients treated with DES and nearly half is attributable to disease progression, which along with the low rate of in-stent restenosis explains why the mode of presentation is often an acute coronary syndrome.
药物洗脱支架(DES)失败包括再狭窄和支架血栓形成,或疾病进展可能导致靶血管血运重建(TVR),但在DES时代这些机制的相对作用尚未得到充分描述。我们试图研究DES术后因临床因素导致TVR的患者的预测因素和临床表现。
分析2004年至2006年动态注册研究中所有接受DES治疗病变的患者。纳入2691例患者的3401处病变。根据基线临床、手术和血管造影特征,比较2年时发生和未发生因临床因素导致TVR的患者,并通过多变量分析确定TVR和靶病变血运重建(TLR)的独立预测因素。
到2年时,7.2%的患者发生TVR,3.8%的患者发生TLR,分别有71.6%和82.5%的再次血运重建事件发生在第一年。首次TVR的指征为心肌梗死占18.6%(n = 34),不稳定型心绞痛占42.6%(n = 78),稳定型冠心病占25.7%(n = 47),其他/不明占13.1%(n = 24)。疾病进展导致47%的TVR。在发生TLR的患者中,再狭窄是机制的占86.6%,支架血栓形成占13.4%。TVR的独立预测因素包括年轻、糖尿病、尝试移植病变、病变长度>30mm和既往病变干预。TVR和TLR的独立预测因素相似。
DES治疗患者中因临床因素导致TVR的发生率较低,近一半归因于疾病进展,这与支架内再狭窄率低共同解释了为什么临床表现模式常为急性冠状动脉综合征。