Section of Breast Oncology, Division of Oncology, Department of Medicine, Washington University School of Medicine, Campus Box 8056, 660 South Euclid Avenue, St. Louis, MO 63110, USA.
Breast Cancer Res Treat. 2013 Jan;137(2):483-92. doi: 10.1007/s10549-012-2378-9. Epub 2012 Dec 15.
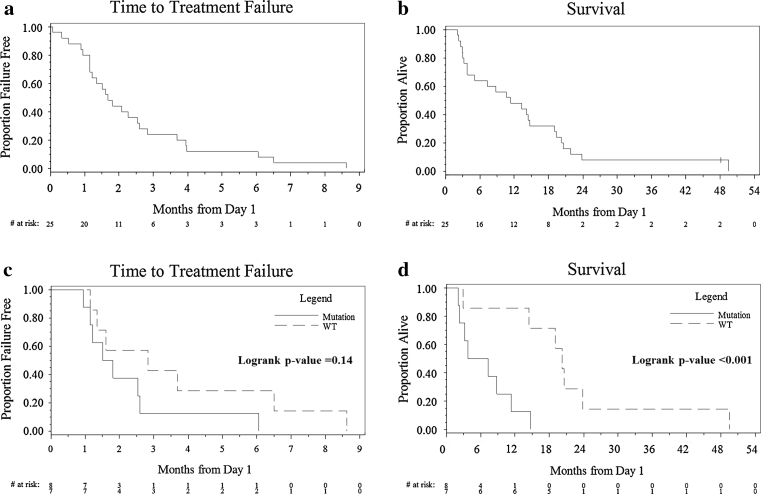
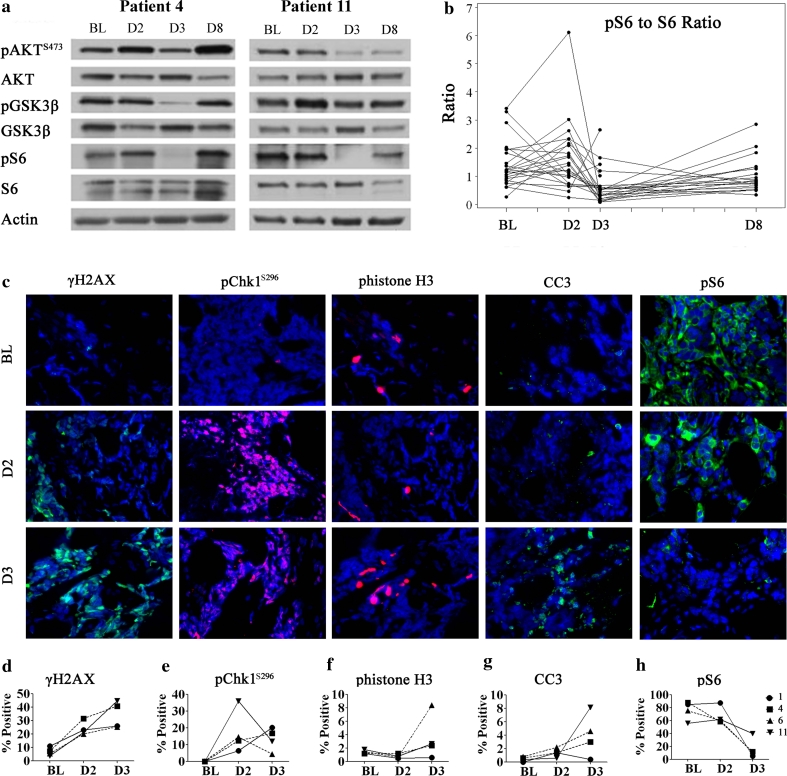
Mutations in TP53 lead to a defective G1 checkpoint and the dependence on checkpoint kinase 1 (Chk1) for G2 or S phase arrest in response to DNA damage. In preclinical studies, Chk1 inhibition resulted in enhanced cytotoxicity of several chemotherapeutic agents. The high frequency of TP53 mutations in triple negative breast cancer (TNBC: negative for estrogen receptor, progesterone receptor, and HER2) make Chk1 an attractive therapeutic target. UCN-01, a non-selective Chk1 inhibitor, combined with irinotecan demonstrated activity in advanced TNBC in our Phase I study. The goal of this trial was to further evaluate this treatment in women with TNBC. Patients with metastatic TNBC previously treated with anthracyclines and taxanes received irinotecan (100-125 mg/m(2) IV days 1, 8, 15, 22) and UCN-01 (70 mg/m(2) IV day 2, 35 mg/m(2) day 23 and subsequent doses) every 42-day cycle. Peripheral blood mononuclear cells (PBMC) and tumor specimens were collected. Twenty five patients were enrolled. The overall response (complete response (CR) + partial response (PR)) rate was 4 %. The clinical benefit rate (CR + PR + stable disease ≥6 months) was 12 %. Since UCN-01 inhibits PDK1, phosphorylated ribosomal protein S6 (pS6) in PBMC was assessed. Although reduced 24 h post UCN-01, pS6 levels rose to baseline by day 8, indicating loss of UCN-01 bioavailability. Immunostains of γH2AX and pChk1(S296) on serial tumor biopsies from four patients demonstrated an induction of DNA damage and Chk1 activation following irinotecan. However, Chk1 inhibition by UCN-01 was not observed in all tumors. Most tumors were basal-like (69 %), and carried mutations in TP53 (53 %). Median overall survival in patients with TP53 mutant tumors was poor compared to wild type (5.5 vs. 20.3 months, p = 0.004). This regimen had limited activity in TNBC. Inconsistent Chk1 inhibition was likely due to the pharmacokinetics of UCN-01. TP53 mutations were associated with a poor prognosis in metastatic TNBC.
TP53 基因突变导致 G1 检验点缺陷,并使细胞对 DNA 损伤的反应依赖于检查点激酶 1(Chk1)而停留在 G2 或 S 期。在临床前研究中,Chk1 抑制剂的应用增强了几种化疗药物的细胞毒性。三阴性乳腺癌(TNBC:雌激素受体、孕激素受体和 HER2 阴性)中 TP53 基因突变的高频率使得 Chk1 成为一个有吸引力的治疗靶点。UCN-01,一种非选择性的 Chk1 抑制剂,与伊立替康联合应用在我们的 I 期研究中显示出对晚期 TNBC 的活性。本试验的目的是进一步评估这种治疗方法在 TNBC 患者中的疗效。既往接受过蒽环类和紫杉烷类药物治疗的转移性 TNBC 患者接受伊立替康(100-125mg/m2 IV 第 1、8、15、22 天)和 UCN-01(70mg/m2 IV 第 2 天,第 23 天和随后的剂量为 35mg/m2),每 42 天为一个周期。采集外周血单核细胞(PBMC)和肿瘤标本。共纳入 25 例患者。总缓解率(完全缓解(CR)+部分缓解(PR))为 4%。临床获益率(CR+PR+稳定疾病≥6 个月)为 12%。由于 UCN-01 抑制 PDK1,因此评估了 PBMC 中磷酸化核糖体蛋白 S6(pS6)的情况。虽然 UCN-01 给药后 24 小时 pS6 水平降低,但第 8 天恢复到基线,表明 UCN-01 的生物利用度丧失。对 4 例患者的连续肿瘤活检进行免疫组化染色显示,伊立替康诱导 DNA 损伤和 Chk1 激活。然而,并非所有肿瘤均观察到 UCN-01 对 Chk1 的抑制作用。大多数肿瘤为基底样(69%),且携带 TP53 基因突变(53%)。TP53 突变型肿瘤患者的总生存期明显短于野生型(5.5 与 20.3 个月,p=0.004)。该方案在 TNBC 中的活性有限。Chk1 抑制作用的不一致可能是由于 UCN-01 的药代动力学所致。TP53 突变与转移性 TNBC 的不良预后相关。