Landry Ian, Sumbly Vikram, Vest Mallorie
Medicine, Icahn School of Medicine at Mount Sinai, New York City Health and Hospitals/Queens, Jamaica, USA.
Internal Medicine, Icahn School of Medicine at Mount Sinai, New York City Health and Hospitals/Queens, Jamaica, USA.
Cureus. 2022 Feb 7;14(2):e21970. doi: 10.7759/cureus.21970. eCollection 2022 Feb.
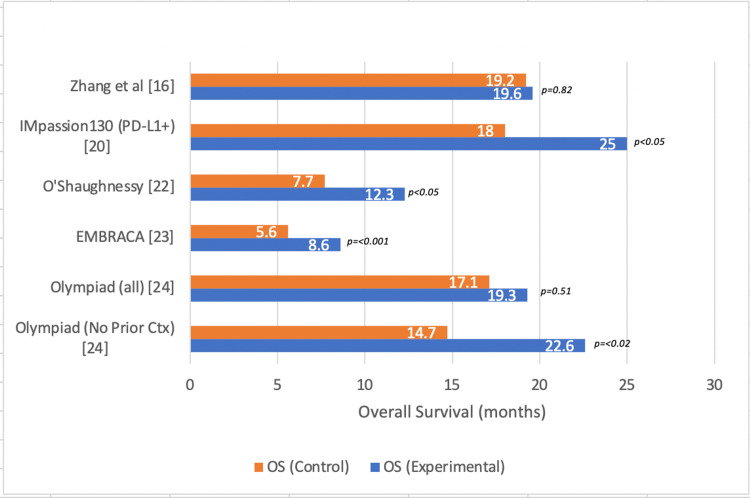
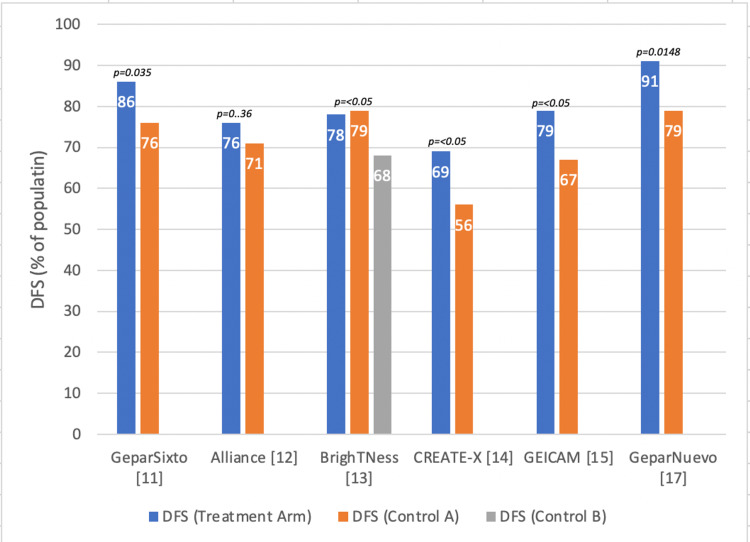
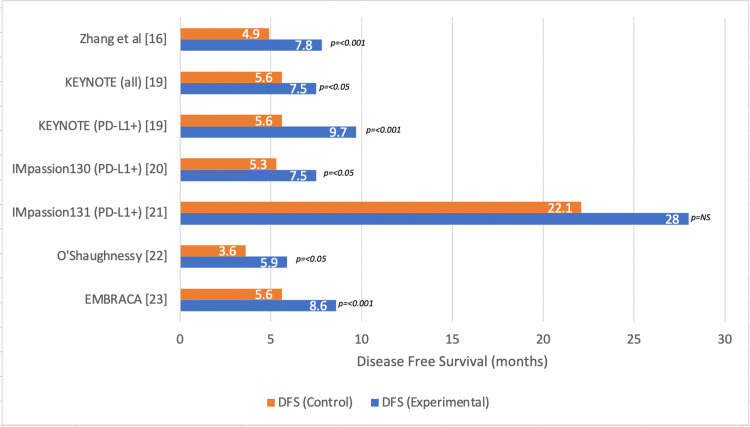
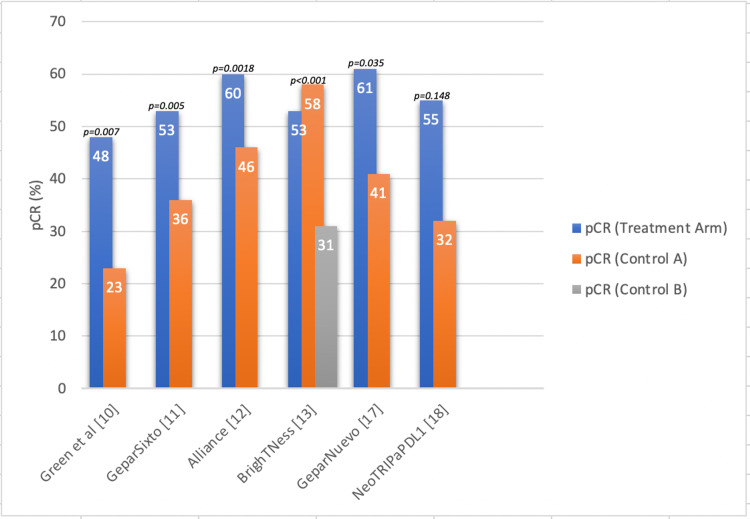
Triple-negative breast cancers (TNBCs) are aggressive tumors that are more common in young women, African American populations, and those with hereditary mutations. These tumors are notable for their high recurrence rate and predilection for chemoresistance. The goal of this narrative review is to describe the current treatment options for patients diagnosed with TNBC and to review the studies that have put forward these recommendations. We searched PubMed and Cochrane databases for free full-text, English-language studies published within the last several years pertaining to the search items "triple negative breast cancer" and "treatment". We included clinical trials and retrospective reviews that had clear designs and assessed their findings against a gold standard or placebo and included evidence of overall response and/or survival outcomes. Patients with early-stage (I-III) TNBC still benefit from treatment with chemotherapeutic regimens involving anthracyclines, taxanes, and antimetabolites. Platinum-based therapies have been shown to improve the overall pathologic complete response (pCR), but there is conflicting evidence with regard to their contribution to disease-free survival (DFS) and overall survival (OS), even with the addition of a poly (ADP-ribose) polymerase (PARP) inhibitor. Patients with residual disease after neoadjuvant chemotherapy and surgical intervention have shown a significant improvement in OS when treated with adjuvant capecitabine. The high mutation burden in metastatic TNBC (mTNBC) allows for targeted therapies and immune checkpoint inhibitors. mTNBCs that express programmed death ligand-1 (PD-L1) receptors may achieve improved response and survival if their regimen includes a monoclonal antibody. Antibody-drug conjugates (ADCs) can deliver high doses of chemotherapy and significantly impact survival in mTNBC regardless of the level of biomarkers expressed by the tumor cells. PARP inhibitors significantly improve survival in newly diagnosed, treatment-naive mTNBC, but have shown mixed results in patients with a history of previous therapy. PARP inhibitors may also target patients with somatic breast cancer (BRCA) and partner and localizer of BRCA-2 (PALB2) mutations, which would allow for more options in this subset of patients. While other rare targets have shown mixed results, the future of treatment may lie in anti-androgen therapy or the development of cancer vaccinations that may increase the immunogenicity of the tumor environment. The management of TNBC includes treatment with multimodal chemotherapy, immune checkpoint inhibitors, and ADCs. The optimal approach depends on a multitude of factors, which include the stage of the tumor, its unique mutational burden, comorbid conditions, and the functional status of the patient. Physicians should be familiar with the advantages and disadvantages of each therapy in order to appropriately counsel and guide their patients.
三阴性乳腺癌(TNBC)是侵袭性肿瘤,在年轻女性、非裔美国人以及有遗传突变的人群中更为常见。这些肿瘤以高复发率和对化疗耐药的倾向而著称。本叙述性综述的目的是描述诊断为TNBC患者的当前治疗选择,并回顾提出这些建议的研究。我们在PubMed和Cochrane数据库中搜索了过去几年内发表的关于搜索词“三阴性乳腺癌”和“治疗”的免费全文、英文研究。我们纳入了设计明确且将其结果与金标准或安慰剂进行比较、并包括总体反应和/或生存结果证据的临床试验和回顾性综述。早期(I - III期)TNBC患者仍受益于含蒽环类、紫杉烷类和抗代谢物的化疗方案治疗。铂类疗法已显示可提高总体病理完全缓解率(pCR),但关于其对无病生存期(DFS)和总生存期(OS)的贡献存在相互矛盾的证据,即使添加了聚(ADP - 核糖)聚合酶(PARP)抑制剂也是如此。新辅助化疗和手术干预后有残留病灶的患者接受辅助卡培他滨治疗时,OS有显著改善。转移性TNBC(mTNBC)的高突变负荷使得靶向治疗和免疫检查点抑制剂成为可能。表达程序性死亡配体 - 1(PD - L1)受体的mTNBC如果其治疗方案包括单克隆抗体,可能会有更好的反应和生存期。抗体 - 药物偶联物(ADC)可递送高剂量化疗药物,并且无论肿瘤细胞表达的生物标志物水平如何,都能显著影响mTNBC的生存期。PARP抑制剂可显著提高新诊断、未接受过治疗的mTNBC患者的生存期,但在既往有治疗史的患者中结果不一。PARP抑制剂也可能适用于患有体细胞乳腺癌(BRCA)和BRCA - 2伴侣及定位蛋白(PALB2)突变的患者,这将为该亚组患者提供更多选择。虽然其他罕见靶点的结果不一,但治疗的未来可能在于抗雄激素治疗或开发可能增加肿瘤环境免疫原性的癌症疫苗。TNBC的管理包括多模式化疗、免疫检查点抑制剂和ADC治疗。最佳方法取决于多种因素,包括肿瘤分期、其独特的突变负荷、合并症以及患者的功能状态。医生应熟悉每种治疗方法的优缺点,以便适当地为患者提供咨询和指导。