Institute for Ethics and Communication in Healthcare Systems, School of Medicine, Faculty of Health, Witten/Herdecke University, Alfred-Herrhausen-Straße 50, D-58448, Witten, Germany.
BMC Med Educ. 2013 Jan 4;13:1. doi: 10.1186/1472-6920-13-1.
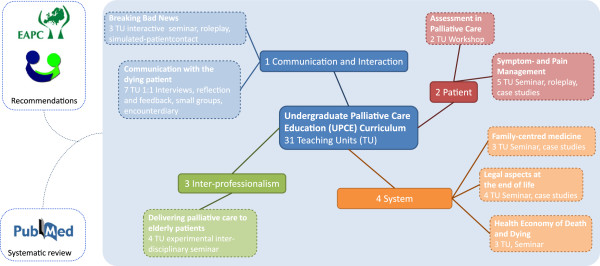
By 2013 Palliative Care will become a mandatory examination subject in the medical curriculum in Germany. There is a pressing need for effective and well-designed curricula and assessment methods. Debates are on going as how Undergraduate Palliative Care Education (UPCE) should be taught and how knowledge and skills should be assessed. It is evident by this time that the development process of early curricula in the US and UK has led to a plethora of diverse curricula which seem to be partly ineffective in improving the care for the seriously ill and dying offered by newly qualified doctors, as is demonstrated in controlled evaluations. The goals of this study were to demonstrate an evidence-based approach towards developing UPCE curricula and investigate the change in medical students' self-perceived readiness to deal with palliative care patients and their families.
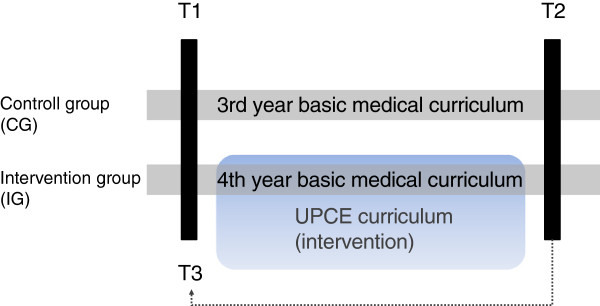
To evaluate the effects of the UPCE curriculum we chose a prospective, controlled, quasi-experimental, pre, retrospective-pre, post study design. A total of n = 37 3rd and 4th -year medical students were assigned to the intervention group (n = 15; 4th -year) and to the control group (n = 22; 3rd-year). Resting on the self-efficacy concept of Bandura the measurement was conducted by a refined test-battery based on two independent measurements (the revised Collet-Lester-Fear-of-Death-Scale and the instrument of the "Program in Palliative Care Education and Practice" at Harvard Medical School) including 68 items altogether in a five-point Likert-scale. These items were designed to test elementary skills in caring for the dying and their relatives as perceived by medical undergraduates. Datasets from both groups were analysed by paired and independent two-sample t-test. The TREND statement for reporting non-randomized evaluations was applied for reporting on this quasi-experimental study.
Three constructs showed statistically significant differences comparing the intervention group before and after. Willingness to accompany a dying patient increased from 21.40 to 37.30 (p < .001). Self-estimation of competence in communication with dying patients and their relatives increased from 12.00 to 23.60 (p = .001). Finally, self-estimation of knowledge and skills in Palliative Care increased from 8.30 to 13.20 (p = .001).
This study is a small but systematic step towards rigorous curricular development in palliative care. Our manualised curriculum is available for scrutiny and scientific feedback to support an open and constructive process of best-practice comparison in palliative care.
到 2013 年,姑息治疗将成为德国医学课程的必修考试科目。因此,我们迫切需要有效的、精心设计的课程和评估方法。目前,人们仍在争论本科生姑息治疗教育(UPCE)应该如何教授,以及应该如何评估知识和技能。此时,人们已经清楚地认识到,美国和英国早期课程的发展过程导致了大量不同的课程,这些课程在改善新资格医生对重病和临终患者的护理方面似乎部分无效,正如对照评估所表明的那样。本研究的目的是展示一种循证方法来开发 UPCE 课程,并调查医学生自我感知处理姑息治疗患者及其家属的能力的变化。
为了评估 UPCE 课程的效果,我们选择了一种前瞻性、对照、准实验、预回顾前、后研究设计。共有 37 名三年级和四年级的医学生被分配到干预组(n=15;四年级)和对照组(n=22;三年级)。基于班杜拉的自我效能概念,我们使用基于两个独立测量的改良测试包进行测量(修订后的科莱特-莱斯特-死亡恐惧量表和哈佛医学院姑息治疗教育与实践计划的工具),包括 68 项五点李克特量表。这些项目旨在测试医学生对临终患者及其亲属护理的基本技能。对两组数据集进行配对和独立两样本 t 检验分析。对这项准实验研究采用了 TRND 报告非随机评估的声明。
在干预组前后比较中,有三个结构显示出统计学上的显著差异。愿意陪伴临终患者的意愿从 21.40 增加到 37.30(p<.001)。与临终患者及其家属沟通的自我估计能力从 12.00 增加到 23.60(p=.001)。最后,姑息治疗知识和技能的自我评估从 8.30 增加到 13.20(p=.001)。
本研究是姑息治疗中严格课程开发的一个小而系统的步骤。我们的规范化课程可供审查和科学反馈,以支持姑息治疗中最佳实践比较的开放和建设性过程。